
Liz Szabo: COVID's silver lining may be breakthroughs against other severe diseases

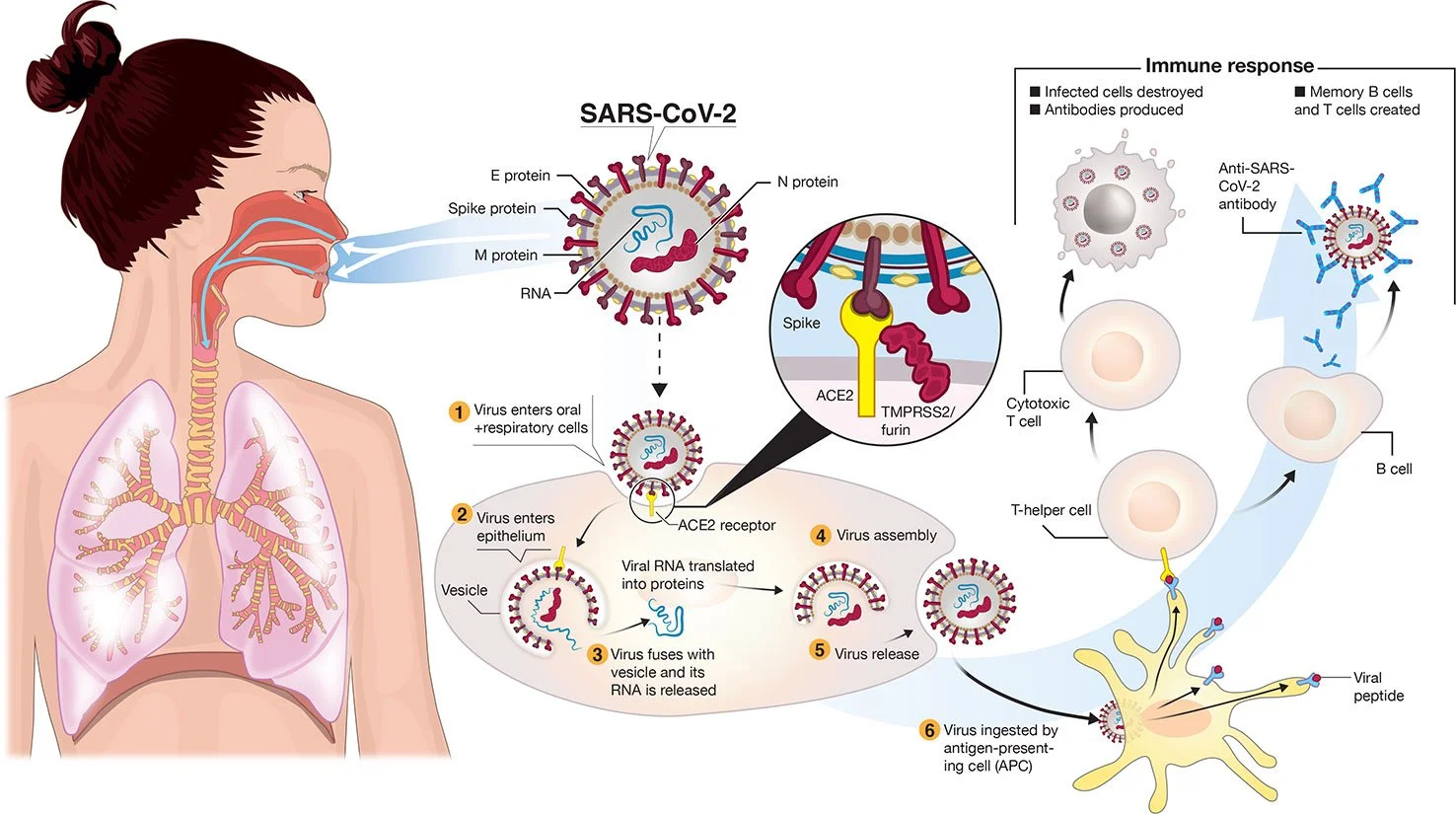
Transmission and life-cycle of SARS-CoV-2 causing COVID-19. 2/furin. A simplified depiction of the life cycle of the virus is shown along with potential immune responses elicited.
— Colin D. Funk, Craig Laferrière, and Ali Ardakani. Graphic by Ian Dennis - http://www.iandennisgraphics.com
“It’s not either/or. We’ve created this artificial dichotomy about how we think about these viruses. But we always put out a mixture of both” when we breathe, cough and sneeze.
— Dr. Michael Klompas, a professor at Harvard Medical School and infectious- disease doctor.
xxx
“There is a lot of frustration about being written off by the medical community, being told that it’s all in one’s head, that they just need to see a psychiatrist or go to the gym.’’
— Dr. David Systrom, a pulmonary and critical-care physician at Brigham and Women’s Hospital, in Boston.
The billions of dollars invested in COVID-19 vaccines and research so far are expected to yield medical and scientific dividends for decades, helping doctors battle influenza, cancer, cystic fibrosis and far more diseases.
“This is just the start,” said Dr. Judith James, vice president of clinical affairs for the Oklahoma Medical Research Foundation. “We won’t see these dividends in their full glory for years.”
Building on the success of mRNA vaccines for covid, scientists hope to create mRNA-based vaccines against a host of pathogens, including influenza, Zika, rabies, HIV, and respiratory syncytial virus, or RSV, which hospitalizes 3 million children under age 5 each year worldwide.
Researchers see promise in mRNA to treat cancer, cystic fibrosis and rare, inherited metabolic disorders, although potential therapies are still many years away.
Pfizer and Moderna worked on mRNA vaccines for cancer long before they developed covid shots. Researchers are now running dozens of clinical trials of therapeutic mRNA vaccines for pancreatic cancer, colorectal cancer, and melanoma, which frequently responds well to immunotherapy.
Companies looking to use mRNA to treat cystic fibrosis include ReCode Therapeutics, Arcturus Therapeutics, and Moderna and Vertex Pharmaceuticals, which are collaborating. The companies’ goal is to correct a fundamental defect in cystic fibrosis, a mutated protein.
Rather than replace the protein itself, scientists plan to deliver mRNA that would instruct the body to make the normal, healthy version of the protein, said David Lockhart, ReCode’s president and chief science officer.
None of these drugs is in clinical trials yet.
That leaves patients such as Nicholas Kelly waiting for better treatment options.
Kelly, 35, was diagnosed with cystic fibrosis as an infant and has never been healthy enough to work full time. He was recently hospitalized for 2½ months due to a lung infection, a common complication for the 30,000 Americans with the disease. Although novel medications have transformed the lives of most people with CF, they don’t work in 10% of patients. About one-third of patients who don’t benefit from the new medications are Black and/or Hispanic, said JP Clancy, vice president of clinical research for the Cystic Fibrosis Foundation.
“Nobody wants to be hospitalized,” said Kelly, who lives in Cleveland. “If something could decrease my symptoms even 10%, I would try it.”
Predicting Which COVID Patients Are Most Likely to Die
Ambitious scientific endeavors have provided technological windfalls for consumers in the past; the race to land on the moon in the 1960s led to the development of CT scanners and MRI machines, freeze-dried food, wireless headphones, water purification systems, and the computer mouse.
Likewise, funding for AIDS research has benefited patients with a variety of diseases, said Dr. Carlos del Rio, a professor of infectious diseases at Emory University School of Medicine. Studies of HIV led to the development of better drugs for hepatitis C and cytomegalovirus, or CMV; paved the way for successful immunotherapies in cancer; and speeded the development of covid vaccines.
Over the past two years, medical researchers have generated more than 230,000 medical journal articles, documenting studies of vaccines, antivirals, and other drugs, as well as basic research into the structure of the virus and how it evades the immune system.
Dr. Michelle Monje, a professor of neurology at Stanford University, has found similarities in the cognitive side effects caused by COVID and a side effect of cancer therapy often called “chemo brain.” Learning more about the root causes of these memory problems, Monje said, could help scientists eventually find ways to prevent or treat them.
James hopes that computer technology used to detect COVID will improve the treatment of other diseases. For example, researchers have shown that cell-phone apps can help detect potential covid cases by monitoring patients’ self-reported symptoms. James said she wonders if the same technology could predict flare-ups of autoimmune diseases.
“We never dreamed we could have a PCR test that could be done anywhere but a lab,” James said. “Now we can do them at a patient’s bedside in rural Oklahoma. That could help us with rapid testing for other diseases.”
One of the most important pandemic breakthroughs was the discovery that 15 to 20 percent of patients over 70 who die of COVID have rogue antibodies that disable a key part of the immune system. Although antibodies normally protect us from infection, these “autoantibodies” attack a protein called interferon that acts as a first line of defense against viruses.
By disabling key immune fighters, autoantibodies against interferon allow the coronavirus to multiply wildly. The massive infection that results can lead the rest of the immune system to go into hyperdrive, causing a life-threatening “cytokine storm,” said Dr. Paul Bastard, a researcher at Rockefeller University.
The discovery of interferon-targeting antibodies “certainly changed my way of thinking at a broad level,” said E. John Wherry, director of the University of Pennsylvania’s Institute for Immunology, who was not involved in the studies. “This is a paradigm shift in immunology and in COVID.”
Antibodies that disable interferon may explain why a fraction of patients succumb to viral diseases, such as influenza, while most recover, said Dr. Gary Michelson, founder and co-chair of Michelson Philanthropies, a nonprofit that funds medical research and recently gave Bastard its inaugural award in immunology.
The discovery “goes far beyond the impact of COVID-19,” Michelson said. “These findings may have implications in treating patients with other infectious diseases” such as the flu.
Bastard and colleagues have also found that one-third of patients with dangerous reactions to yellow fever have autoantibodies against interferon.
International research teams are now looking for such autoantibodies in patients hospitalized by other viral infections, including chickenpox, influenza, measles, respiratory syncytial virus, and others.
Overturning Dogma
For decades, public health officials created policies based on the assumption that viruses spread in one of two ways: either through the air, like measles and tuberculosis, or through heavy, wet droplets that spray from our mouths and noses, then quickly fall to the ground, like influenza.
For the first 17 months of the covid pandemic, the World Health Organization and the Centers for Disease Control and Prevention said the coronavirus spread through droplets and advised people to wash their hands, stand 6 feet apart, and wear face coverings. As the crisis wore on and evidence accumulated, researchers began to debate whether the coronavirus might also be airborne.
Today it’s clear that the coronavirus — and all respiratory viruses — spread through a combination of droplets and aerosols, said Dr. Michael Klompas, a professor at Harvard Medical School and infectious disease doctor.
“It’s not either/or,” Klompas said. “We’ve created this artificial dichotomy about how we think about these viruses. But we always put out a mixture of both” when we breathe, cough, and sneeze.
Knowing that respiratory viruses commonly spread through the air is important because it can help health agencies protect the public. For example, high-quality masks, such as N95 respirators, offer much better protection against airborne viruses than cloth masks or surgical masks. Improving ventilation, so that the air in a room is completely replaced at least four to six times an hour, is another important way to control airborne viruses.
Still, Klompas said, there’s no guarantee that the country will handle the next outbreak any better than this one. “Will we do a better job fighting influenza because of what we’ve learned?” Klompas said. “I hope so, but I’m not holding my breath.”
Fighting Chronic Disease
Lauren Nichols, 32, remembers exactly when she developed her first covid symptoms: March 10, 2020.
It was the beginning of an illness that has plagued her for nearly two years, with no end in sight. Although Nichols was healthy before developing what has become known as “long COVID,” she deals with dizziness, headaches, and debilitating fatigue, which gets markedly worse after exercise. She has had shingles — a painful rash caused by the reactivation of the chickenpox virus — four times since her covid infection.
Six months after testing positive for COVID, Nichols was diagnosed with chronic fatigue syndrome, also known as myalgic encephalomyelitis, or ME/CFS, which affects more than 1 million Americans and causes many of the same symptoms as COVID. There are few effective treatments for either condition.
In fact, research suggests that “the two conditions are one and the same,” said Dr. Avindra Nath, clinical director of the National Institute of Neurological Disorders and Stroke, part of the National Institutes of Health. The main difference is that people with long COVID know which virus caused their illness, while the precise virus behind most cases of chronic fatigue is unknown, Nath said.
Advocates of patients with long COVID want to ensure that future research — including $1.15 billion in targeted funding from the NIH — benefits all patients with chronic, post-viral diseases.
“Anything that shows promise in long covid will be immediately trialed in ME/CFS,” said Jarred Younger, director of the Neuroinflammation, Pain and Fatigue Laboratory at the University of Alabama-Birmingham.
Patients with chronic fatigue syndrome have felt a kinship with long COVID patients, and vice versa, not just because they experience the same baffling symptoms, but also because both have struggled to obtain compassionate, appropriate care, said Nichols, vice president of Body Politic, an advocacy group for people with long COVID and other chronic or disabling conditions.
“There is a lot of frustration about being written off by the medical community, being told that it’s all in one’s head, that they just need to see a psychiatrist or go to the gym,” said Dr. David Systrom, a pulmonary and critical care physician at Brigham and Women’s Hospital in Boston.
That sort of ignorance seems to be declining, largely because of increasing awareness about long COVID, said Emily Taylor, vice president of advocacy and engagement at Solve M.E., an advocacy group for people with post-infectious chronic illnesses. Although some doctors still refuse to believe long covid is a real disease, “they’re being drowned out by the patient voices,” Taylor said.
A new study from the National Institutes of Health, called RECOVER (Researching COVID to Enhance Recovery), is enrolling 15,000 people with long covid and a comparison group of nearly 3,000 others who haven’t had covid.
“In a very dark cloud,” Nichols said, “a silver lining coming out of long covid is that we’ve been forced to acknowledge how real and serious these conditions are.”
Liz Szabo is a Kaiser Health News reporter.