
Liz Szabo: COVID's silver lining may be breakthroughs against other severe diseases

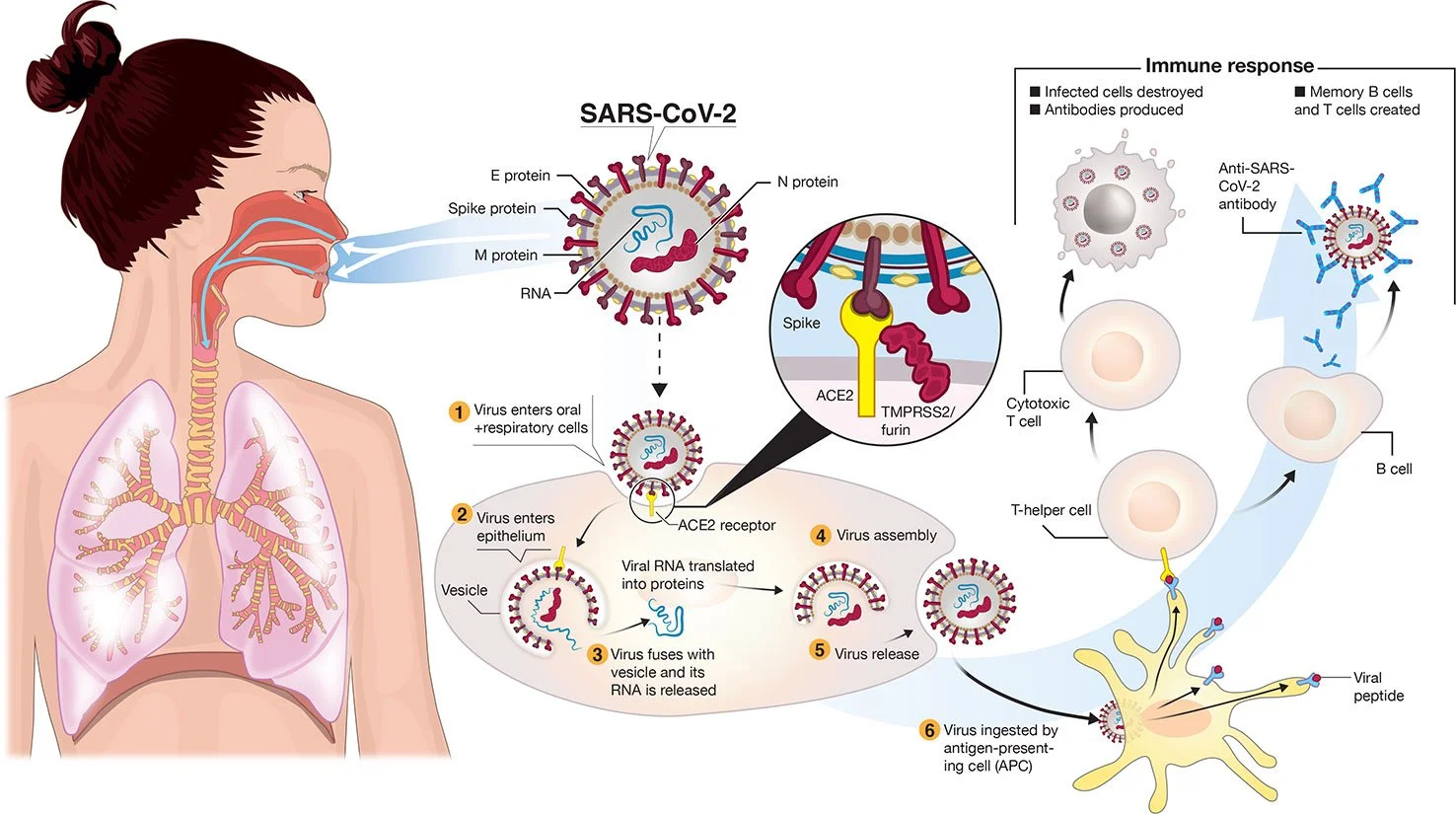
Transmission and life-cycle of SARS-CoV-2 causing COVID-19. 2/furin. A simplified depiction of the life cycle of the virus is shown along with potential immune responses elicited.
— Colin D. Funk, Craig Laferrière, and Ali Ardakani. Graphic by Ian Dennis - http://www.iandennisgraphics.com
“It’s not either/or. We’ve created this artificial dichotomy about how we think about these viruses. But we always put out a mixture of both” when we breathe, cough and sneeze.
— Dr. Michael Klompas, a professor at Harvard Medical School and infectious- disease doctor.
xxx
“There is a lot of frustration about being written off by the medical community, being told that it’s all in one’s head, that they just need to see a psychiatrist or go to the gym.’’
— Dr. David Systrom, a pulmonary and critical-care physician at Brigham and Women’s Hospital, in Boston.
The billions of dollars invested in COVID-19 vaccines and research so far are expected to yield medical and scientific dividends for decades, helping doctors battle influenza, cancer, cystic fibrosis and far more diseases.
“This is just the start,” said Dr. Judith James, vice president of clinical affairs for the Oklahoma Medical Research Foundation. “We won’t see these dividends in their full glory for years.”
Building on the success of mRNA vaccines for covid, scientists hope to create mRNA-based vaccines against a host of pathogens, including influenza, Zika, rabies, HIV, and respiratory syncytial virus, or RSV, which hospitalizes 3 million children under age 5 each year worldwide.
Researchers see promise in mRNA to treat cancer, cystic fibrosis and rare, inherited metabolic disorders, although potential therapies are still many years away.
Pfizer and Moderna worked on mRNA vaccines for cancer long before they developed covid shots. Researchers are now running dozens of clinical trials of therapeutic mRNA vaccines for pancreatic cancer, colorectal cancer, and melanoma, which frequently responds well to immunotherapy.
Companies looking to use mRNA to treat cystic fibrosis include ReCode Therapeutics, Arcturus Therapeutics, and Moderna and Vertex Pharmaceuticals, which are collaborating. The companies’ goal is to correct a fundamental defect in cystic fibrosis, a mutated protein.
Rather than replace the protein itself, scientists plan to deliver mRNA that would instruct the body to make the normal, healthy version of the protein, said David Lockhart, ReCode’s president and chief science officer.
None of these drugs is in clinical trials yet.
That leaves patients such as Nicholas Kelly waiting for better treatment options.
Kelly, 35, was diagnosed with cystic fibrosis as an infant and has never been healthy enough to work full time. He was recently hospitalized for 2½ months due to a lung infection, a common complication for the 30,000 Americans with the disease. Although novel medications have transformed the lives of most people with CF, they don’t work in 10% of patients. About one-third of patients who don’t benefit from the new medications are Black and/or Hispanic, said JP Clancy, vice president of clinical research for the Cystic Fibrosis Foundation.
“Nobody wants to be hospitalized,” said Kelly, who lives in Cleveland. “If something could decrease my symptoms even 10%, I would try it.”
Predicting Which COVID Patients Are Most Likely to Die
Ambitious scientific endeavors have provided technological windfalls for consumers in the past; the race to land on the moon in the 1960s led to the development of CT scanners and MRI machines, freeze-dried food, wireless headphones, water purification systems, and the computer mouse.
Likewise, funding for AIDS research has benefited patients with a variety of diseases, said Dr. Carlos del Rio, a professor of infectious diseases at Emory University School of Medicine. Studies of HIV led to the development of better drugs for hepatitis C and cytomegalovirus, or CMV; paved the way for successful immunotherapies in cancer; and speeded the development of covid vaccines.
Over the past two years, medical researchers have generated more than 230,000 medical journal articles, documenting studies of vaccines, antivirals, and other drugs, as well as basic research into the structure of the virus and how it evades the immune system.
Dr. Michelle Monje, a professor of neurology at Stanford University, has found similarities in the cognitive side effects caused by COVID and a side effect of cancer therapy often called “chemo brain.” Learning more about the root causes of these memory problems, Monje said, could help scientists eventually find ways to prevent or treat them.
James hopes that computer technology used to detect COVID will improve the treatment of other diseases. For example, researchers have shown that cell-phone apps can help detect potential covid cases by monitoring patients’ self-reported symptoms. James said she wonders if the same technology could predict flare-ups of autoimmune diseases.
“We never dreamed we could have a PCR test that could be done anywhere but a lab,” James said. “Now we can do them at a patient’s bedside in rural Oklahoma. That could help us with rapid testing for other diseases.”
One of the most important pandemic breakthroughs was the discovery that 15 to 20 percent of patients over 70 who die of COVID have rogue antibodies that disable a key part of the immune system. Although antibodies normally protect us from infection, these “autoantibodies” attack a protein called interferon that acts as a first line of defense against viruses.
By disabling key immune fighters, autoantibodies against interferon allow the coronavirus to multiply wildly. The massive infection that results can lead the rest of the immune system to go into hyperdrive, causing a life-threatening “cytokine storm,” said Dr. Paul Bastard, a researcher at Rockefeller University.
The discovery of interferon-targeting antibodies “certainly changed my way of thinking at a broad level,” said E. John Wherry, director of the University of Pennsylvania’s Institute for Immunology, who was not involved in the studies. “This is a paradigm shift in immunology and in COVID.”
Antibodies that disable interferon may explain why a fraction of patients succumb to viral diseases, such as influenza, while most recover, said Dr. Gary Michelson, founder and co-chair of Michelson Philanthropies, a nonprofit that funds medical research and recently gave Bastard its inaugural award in immunology.
The discovery “goes far beyond the impact of COVID-19,” Michelson said. “These findings may have implications in treating patients with other infectious diseases” such as the flu.
Bastard and colleagues have also found that one-third of patients with dangerous reactions to yellow fever have autoantibodies against interferon.
International research teams are now looking for such autoantibodies in patients hospitalized by other viral infections, including chickenpox, influenza, measles, respiratory syncytial virus, and others.
Overturning Dogma
For decades, public health officials created policies based on the assumption that viruses spread in one of two ways: either through the air, like measles and tuberculosis, or through heavy, wet droplets that spray from our mouths and noses, then quickly fall to the ground, like influenza.
For the first 17 months of the covid pandemic, the World Health Organization and the Centers for Disease Control and Prevention said the coronavirus spread through droplets and advised people to wash their hands, stand 6 feet apart, and wear face coverings. As the crisis wore on and evidence accumulated, researchers began to debate whether the coronavirus might also be airborne.
Today it’s clear that the coronavirus — and all respiratory viruses — spread through a combination of droplets and aerosols, said Dr. Michael Klompas, a professor at Harvard Medical School and infectious disease doctor.
“It’s not either/or,” Klompas said. “We’ve created this artificial dichotomy about how we think about these viruses. But we always put out a mixture of both” when we breathe, cough, and sneeze.
Knowing that respiratory viruses commonly spread through the air is important because it can help health agencies protect the public. For example, high-quality masks, such as N95 respirators, offer much better protection against airborne viruses than cloth masks or surgical masks. Improving ventilation, so that the air in a room is completely replaced at least four to six times an hour, is another important way to control airborne viruses.
Still, Klompas said, there’s no guarantee that the country will handle the next outbreak any better than this one. “Will we do a better job fighting influenza because of what we’ve learned?” Klompas said. “I hope so, but I’m not holding my breath.”
Fighting Chronic Disease
Lauren Nichols, 32, remembers exactly when she developed her first covid symptoms: March 10, 2020.
It was the beginning of an illness that has plagued her for nearly two years, with no end in sight. Although Nichols was healthy before developing what has become known as “long COVID,” she deals with dizziness, headaches, and debilitating fatigue, which gets markedly worse after exercise. She has had shingles — a painful rash caused by the reactivation of the chickenpox virus — four times since her covid infection.
Six months after testing positive for COVID, Nichols was diagnosed with chronic fatigue syndrome, also known as myalgic encephalomyelitis, or ME/CFS, which affects more than 1 million Americans and causes many of the same symptoms as COVID. There are few effective treatments for either condition.
In fact, research suggests that “the two conditions are one and the same,” said Dr. Avindra Nath, clinical director of the National Institute of Neurological Disorders and Stroke, part of the National Institutes of Health. The main difference is that people with long COVID know which virus caused their illness, while the precise virus behind most cases of chronic fatigue is unknown, Nath said.
Advocates of patients with long COVID want to ensure that future research — including $1.15 billion in targeted funding from the NIH — benefits all patients with chronic, post-viral diseases.
“Anything that shows promise in long covid will be immediately trialed in ME/CFS,” said Jarred Younger, director of the Neuroinflammation, Pain and Fatigue Laboratory at the University of Alabama-Birmingham.
Patients with chronic fatigue syndrome have felt a kinship with long COVID patients, and vice versa, not just because they experience the same baffling symptoms, but also because both have struggled to obtain compassionate, appropriate care, said Nichols, vice president of Body Politic, an advocacy group for people with long COVID and other chronic or disabling conditions.
“There is a lot of frustration about being written off by the medical community, being told that it’s all in one’s head, that they just need to see a psychiatrist or go to the gym,” said Dr. David Systrom, a pulmonary and critical care physician at Brigham and Women’s Hospital in Boston.
That sort of ignorance seems to be declining, largely because of increasing awareness about long COVID, said Emily Taylor, vice president of advocacy and engagement at Solve M.E., an advocacy group for people with post-infectious chronic illnesses. Although some doctors still refuse to believe long covid is a real disease, “they’re being drowned out by the patient voices,” Taylor said.
A new study from the National Institutes of Health, called RECOVER (Researching COVID to Enhance Recovery), is enrolling 15,000 people with long covid and a comparison group of nearly 3,000 others who haven’t had covid.
“In a very dark cloud,” Nichols said, “a silver lining coming out of long covid is that we’ve been forced to acknowledge how real and serious these conditions are.”
Liz Szabo is a Kaiser Health News reporter.

Don Pesci: In the pandemic, separating science and political science

Treating a patient on a ventilator in a hospital’s intensive-care unit
VERNON, Conn.
How scientific is science in the matter of Coronavirus?
There’s science and there’s political science. The one thing we do not want in any confluence of the two is confusion and mass hysteria, which can best be avoided by observing this rule: Politicians should decide political matters and medical scientists should decide medical matters. Occasionally, politicians decide that mass fright can better able convince the general population than rational argument.
The answer to the above question is simple: In the case of new viruses, science, as defined above, must be silent. There can be no “scientific” view of Coronavirus because it is a new phenomenon, the recent arrival of a stranger on the medical block. Concerning Coronavirus, there are, properly speaking, multiple views of different scientists, many of whom will disagree with each other on important points.
Does Coronavirus remain on surfaces for long periods? A couple of months ago, we were told by politicians, relaying the news from “science”, that hard surfaces were repositories of Coronavirus, and that contamination from hard surfaces was as likely as person-to-person contamination. That notion has withered on the vine now that we know Coronavirus is most often spread person to person.
Do adults spread Coronavirus to children, or are children the Bloody Marys? This is an important datum because if children, who are much less likely than adults to die or be seriously ill from Coronavirus, spread the virus to adults, the wholesale closing of schools might be a protective measure.
But if adults pass the virus to children, the current view of many scientists, remediation efforts would be far different. We are told that love covers a multitude of sins including, Agatha Christie advises us, murder. The word “science” misapplied covers, we have seen, a multitude of political sins.If we can learn from our past mistakes, we need not carry our mistakes into the future.
If the question is, “Have politicians in the Northeast made a mistake in trusting to some scientists?” the question is wrongly put. It’s not quite as simple as that. It will always be better to take advice from the horse’s mouth rather than from the horse’s posterior. But in the process, politicians must not allow differing scientists to determine the political course of a state.
Politicians, in the face of a pandemic, should not stop being politicians. That is what we have seen in Northeast states, where Coronavirus has dug in its heels. Here legislative activity has been shut down, and Connecticut Gov. Ned Lamont has been festooned with extraordinary – some would say unconstitutional -- powers.
Like his counterpart in New York, Andrew Cuomo, Lamont has resorted to state-wide business shutdowns and sequestration. But inducing a long-lived recession in Connecticut, sequestration and data collection are not curative, however “necessary” they seem to be to some politicians who are masters in the art of spreading fear.
A vaccine may cure Coronavirus. What is called herd-immunity may reduce infestation. Certain people, in many cases younger people, catch the virus and develop a natural immunity, foreshortening the mass of people fatally exposed to the virus. We know that Coronavirus has spread like a wildfire in nursing homes, because clients in nursing homes are older and subject to other infirmities that in their cases have dramatically increased the fatality rate in Connecticut and New York.
“Science” – real science – warned us of this at the very beginning of the infestation. We knew of a certainty that older people with compromised systems were especially vulnerable. So, knowing this, why did not the governors of Connecticut and New York direct more of their resources to nursing homes? That is a question that must be answered by our “savior politicians.”
Home sequestration, we have been told, helps to flatten the Coronavirus curve. What can this mean if not that sequestration prolongs the time during which the sequestered may in the future be exposed to the virus? Flattening the curve is not curative. Ask any scientist.
The Coronavirus pandemic has been Hell, but it is very important that we should not return from Hell with empty hands.
In Connecticut more than 60 percent of deaths “associated with” Coronavirus occurred in nursing homes; the figure is similar in New York. Cuomo recently acknowledged he was surprised to discover that a sizable majority of people in New York infected with Coronavirus had been sequestered at home. His surprise is surprising.
We are told that business re-opening will occur in Connecticut in three stages, somewhat like a rocket on its way to the moon. But surely business opening should be determined with reference to sections of Connecticut that have been severely or mildly affected by Coronavirus, and the distribution of Coronavirus throughout the state has been mapped by Johns Hopkins University ever since the virus penetrated the United States from its point of origin, Wuhan, China.
These are political decisions that should have been codified in law by a quiescent General Assembly. Political science – yes, there is such a thing – would tell us that we no longer enjoy in Connecticut a republican, small “r”, constitutional government. Instead, Governor Lamont has become our homegrown Xi Jinping, China’s communist tyrant who has now provided Connecticut both with a deadly virus and PPEs, the means of thwarting some of its effects.
Don Pesci is a Vernon-based columnist.
Elisabeth Rosenthal/ Emmarie Huetteman: He got tested for COVID-19; then came a flood of medical bills
By March 5, Andrew Cencini, a computer-science professor at Vermont’s Bennington College, had been having bouts of fever, malaise and a bit of difficulty breathing for a couple of weeks. Just before falling ill, he had traveled to New York City, helped with computers at a local prison and gone out on multiple calls as a volunteer firefighter.
So with COVID-19 cases rising across the country, he called his doctor for direction. He was advised to come to the doctor’s group practice, where staff took swabs for flu and other viruses as he sat in his truck. The results came back negative.

In an isolation room, the doctors put Andrew Cencini on an IV drip, did a chest X-ray and took the swabs.
— Photo courtesy of Andrew Cencini
By March 9, he reported to his doctor that he was feeling better but still had some cough and a low-grade fever. Within minutes, he got a call from the heads of a hospital emergency room and infectious-disease department where he lives in upstate New York: He should come right away to the ER for newly available coronavirus testing. Though they offered to send an ambulance, he felt fine and drove the hourlong trip.
In an isolation room, the doctors put him on an IV drip, did a chest X-ray and took the swabs.
Now back at work remotely, he faces a mounting array of bills. His patient responsibility, according to his insurer, is close to $2,000, and he fears there may be more bills to come.
“I was under the assumption that all that would be covered,” said Cencini, who makes $54,000 a year. “I could have chosen not to do all this, and put countless others at risk. But I was trying to do the right thing.”
The new $2 trillion coronavirus aid package allocates well over $100 billion to what Senate Minority Leader Chuck Schumer of New York called “a Marshall Plan” for hospitals and medical needs.
But no one is doing much to similarly rescue patients from the related financial stress. And they desperately need protection from the kind of bills patients like Cencini are likely to incur in a system that freely charges for every bit of care it dispenses.
On March 18, President Trump signed a law intended to ensure that Americans could be tested for the coronavirus free, whether they have insurance or not. (He had also announced that health insurers have agreed to waive patient copayments for treatment of COVID-19, the disease caused by the virus.) But their published policies vary widely and leave countless ways for patients to get stuck.
Although insurers had indeed agreed to cover the full cost of diagnostic coronavirus tests, that may well prove illusory: Cencini’s test was free, but his visit to the ER to get it was not.
As might be expected in a country where the price of a knee X-ray can vary by a factor of well over 10, labs so far are charging between about $51 (the Medicare reimbursement rate) and more than $100 for the test. How much will insurers cover?
Those testing laboratories want to be paid — and now. Last week, the American Clinical Laboratory Association, an industry group, complained that they were being overlooked in the coronavirus package.
“Collectively, these labs have completed over 234,000 tests to date, and nearly quadrupled our daily test capacity over the past week,” Julie Khani, president of the ACLA, said in a statement. “They are still waiting for reimbursement for tests performed. In many cases, labs are receiving specimens with incomplete or no insurance information, and are burdened with absorbing the cost.”
There are few provisions in the relief packages to ensure that patients will be protected from large medical bills related to testing, evaluation or treatment — especially since so much of it is taking place in a financial high-risk setting for patients: the emergency room.
In a study last year, about 1 in 6 visits to an emergency room or stays in a hospital had at least one out-of-network charge, increasing the risk of patients’ receiving surprise medical bills, many demanding payment from patients.
That is in large part because many in-network emergency rooms are staffed by doctors who work for private companies, which are not in the same networks. In a Texas study, more than 30 percent of ER physician services were out-of-network — and most of those services were delivered at in-network hospitals.
The doctor who saw Cencini works with Emergency Care Services of New York, which provides physicians on contract to hospitals and works with some but not all insurers. It is affiliated with TeamHealth, a medical staffing business owned by the private equity firm Blackstone that has come under fire for generating surprise bills.
Some senators had wanted to put a provision in legislation passed in response to the coronavirus to protect patients from surprise out-of-network billing — either a broad clause or one specifically related to coronavirus care. Lobbyists for hospitals, physician staffing firms and air ambulances apparently helped ensure it stayed out of the final version. They played what a person familiar with the negotiations, who spoke on the condition of anonymity, called “the COVID card”: “How could you possibly ask us to deal with surprise billing when we’re trying to battle this pandemic?”
Even without an ER visit, there are perilous billing risks. Not all hospitals and labs are capable of performing the test. And what if my in-network doctor sends my coronavirus test to an out-of-network lab? Before the pandemic, the Kaiser Health News-NPR “Bill of the Month” project produced a feature about Alexa Kasdan, a New Yorker with a head cold, whose throat swab was sent to an out-of-network lab that billed more than $28,000 for testing.
Even patients who do not contract the coronavirus are at a higher risk of incurring a surprise medical bill during the current crisis, when an unrelated health emergency could land you in an unfamiliar, out-of-network hospital because your hospital is too full of COVID-19 patients.
The coronavirus bills passed so far — and those on the table — offer inadequate protection from a system primed to bill patients for all kinds of costs. The Families First Coronavirus Response Act, passed last month, says the test and its related charges will be covered with no patient charge only to the extent that they are related to administering the test or evaluating whether a patient needs it.
That leaves hospital billers and coders wide berth. Cencini went to the ER to get a test, as he was instructed to do. When he called to protest his $1,622.52 bill for hospital charges (his insurer’s discounted rate from over $2,500 in the hospital’s billed charges), a patient representative confirmed that the ER visit and other services performed would be “eligible for cost-sharing” (in his case, all of it, since he had not met his deductible).
Last weekend he was notified that the physician charge from Emergency Care Services of New York was $1,166. Though “covered” by his insurance, he owes another $321 for that, bringing his out-of-pocket costs to nearly $2,000.
By the way, his test came back negative.
When he got off the phone with his insurer, his blood was “at the boiling point,” he told us. “My retirement account is tanking and I’m expected to pay for this?”
The coronavirus aid package provides a stimulus payment of $1,200 per person for most adults. Thanks to the billing proclivities of the American health care system, that will not fully offset Cencini’s medical bills.
Elisabeth Rosenthal: erosenthal@kff.org, @rosenthalhealth
Emmarie Huetteman: ehuetteman@kff.org, @emmarieDC

On the Bennington College campus on a dreary day