

Michelle Andrews: Fertility treatment can be out of reach for the poor
From Kaiser Family Foundation Health News
“This is really sort of standing out as a sore thumb in a nation that would like to claim that it cares for the less fortunate and it seeks to do anything it can for them.’’
— Eli Adashi, a professor of medical science at Brown University and former president of the Society for Reproductive Endocrinologists.
Mary Delgado’s first pregnancy went according to plan, but when she tried to get pregnant again seven years later, nothing happened. After 10 months, Delgado, now 34, and her partner, Joaquin Rodriguez, went to see an OB-GYN. Tests showed she had endometriosis, which was interfering with conception. Delgado’s only option, the doctor said, was in vitro fertilization.
“When she told me that, she broke me inside,” Delgado said, “because I knew it was so expensive.”
Delgado, who lives in New York City, is enrolled in Medicaid, the federal-state health program for low-income and disabled people. The roughly $20,000 price tag for a round of IVF would be a financial stretch for lots of people, but for someone on Medicaid — for which the maximum annual income for a two-person household in New York is just over $26,000 — the treatment can be unattainable.
Expansions of work-based insurance plans to cover fertility treatments, including free egg freezing and unlimited IVF cycles, are often touted by large companies as a boon for their employees. But people with lower incomes, often minorities, are more likely to be covered by Medicaid or skimpier commercial plans with no such coverage. That raises the question of whether medical assistance to create a family is only for the well-to-do or people with generous benefit packages.
“In American health care, they don’t want the poor people to reproduce,” Delgado said. She was caring full-time for their son, who was born with a rare genetic disorder that required several surgeries before he was 5. Her partner, who works for a company that maintains the city’s yellow cabs, has an individual plan through the state insurance marketplace, but it does not include fertility coverage.
Years after she had her first child, Joaquin , Mary Delgado found out that she had endometriosis and that IVF was her only option to get pregnant again. The news from her doctor “broke me inside,” Delgado says, “because I knew it was so expensive.” Delgado, who is on Medicaid, traveled more than 300 miles round trip for lower-cost IVF, and she and her partner, Joaquin Rodriguez, used savings they’d set aside for a home. Their daughter, Emiliana, is now almost a year old.
Some medical experts whose patients have faced these issues say they can understand why people in Delgado’s situation think the system is stacked against them.
“It feels a little like that,” said Elizabeth Ginsburg, a professor of obstetrics and gynecology at Harvard Medical School who is president-elect of the American Society for Reproductive Medicine, a research and advocacy group.
Whether or not it’s intended, many say the inequity reflects poorly on the U.S.
“This is really sort of standing out as a sore thumb in a nation that would like to claim that it cares for the less fortunate and it seeks to do anything it can for them,” said Eli Adashi, a professor of medical science at Brown University and former president of the Society for Reproductive Endocrinologists.
Yet efforts to add coverage for fertility care to Medicaid face a lot of pushback, Ginsburg said.
Over the years, Barbara Collura, president and CEO of the advocacy group Resolve: The National Infertility Association, has heard many explanations for why it doesn’t make sense to cover fertility treatment for Medicaid recipients. Legislators have asked, “If they can’t pay for fertility treatment, do they have any idea how much it costs to raise a child?” she said.
“So right there, as a country we’re making judgments about who gets to have children,” Collura said.
The legacy of the eugenics movement of the early 20th century, when states passed laws that permitted poor, nonwhite, and disabled people to be sterilized against their will, lingers as well.
“As a reproductive justice person, I believe it’s a human right to have a child, and it’s a larger ethical issue to provide support,” said Regina Davis Moss, president and CEO of In Our Own Voice: National Black Women’s Reproductive Justice Agenda, an advocacy group.
But such coverage decisions — especially when the health care safety net is involved — sometimes require difficult choices, because resources are limited.
Even if state Medicaid programs wanted to cover fertility treatment, for instance, they would have to weigh the benefit against investing in other types of care, including maternity care, said Kate McEvoy, executive director of the National Association of Medicaid Directors. “There is a recognition about the primacy and urgency of maternity care,” she said.
Medicaid pays for about 40 percent of births in the United States. And since 2022, 46 states and the District of Columbia have elected to extend Medicaid postpartum coverage to 12 months, up from 60 days.
Fertility problems are relatively common, affecting roughly 10% of women and men of childbearing age, according to the National Institute of Child Health and Human Development.
Traditionally, a couple is considered infertile if they’ve been trying to get pregnant unsuccessfully for 12 months. Last year, the ASRM broadened the definition of infertility to incorporate would-be parents beyond heterosexual couples, including people who can’t get pregnant for medical, sexual, or other reasons, as well as those who need medical interventions such as donor eggs or sperm to get pregnant.
The World Health Organization defined infertility as a disease of the reproductive system characterized by failing to get pregnant after a year of unprotected intercourse. It terms the high cost of fertility treatment a major equity issue and has called for better policies and public financing to improve access.
No matter how the condition is defined, private health plans often decline to cover fertility treatments because they don’t consider them “medically necessary.” Twenty states and Washington, D.C., have laws requiring health plans to provide some fertility coverage, but those laws vary greatly and apply only to companies whose plans are regulated by the state.
In recent years, many companies have begun offering fertility treatment in a bid to recruit and retain top-notch talent. In 2023, 45 percent of companies with 500 or more workers covered IVF and/or drug therapy, according to the benefits consultant Mercer.
But that doesn’t help people on Medicaid. Only two states’ Medicaid programs provide any fertility treatment: New York covers some oral ovulation-enhancing medications, and Illinois covers costs for fertility preservation, to freeze the eggs or sperm of people who need medical treatment that will likely make them infertile, such as for cancer. Several other states also are considering adding fertility preservation services.
In Delgado’s case, Medicaid covered the tests to diagnose her endometriosis, but nothing more. She was searching the internet for fertility treatment options when she came upon a clinic group called CNY Fertility that seemed significantly less expensive than other clinics, and also offered in-house financing. Based in Syracuse, New York, the company has a handful of clinics in upstate New York cities and four other U.S. locations.
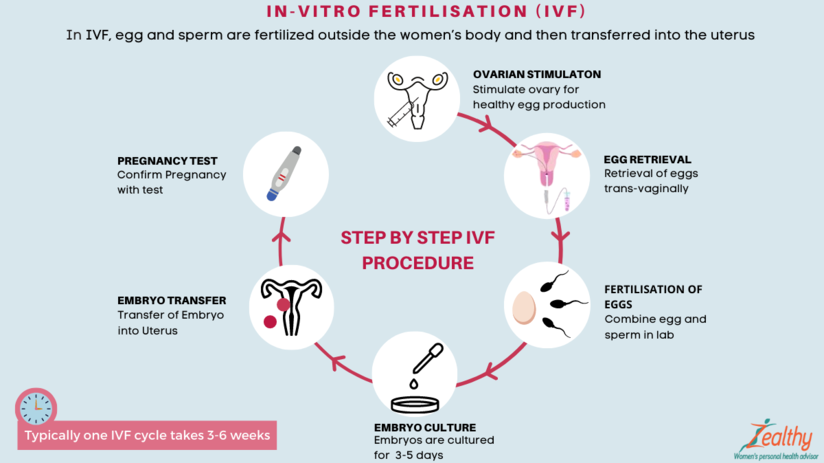
Though Delgado and her partner had to travel more than 300 miles round trip to Albany for the procedures, the savings made it worthwhile. They were able do an entire IVF cycle, including medications, egg retrieval, genetic testing, and transferring the egg to her uterus, for $14,000. To pay for it, they took $7,000 of the cash they’d been saving to buy a home and financed the other half through the fertility clinic.
She got pregnant on the first try, and their daughter, Emiliana, is now almost a year old.
Delgado doesn’t resent people with more resources or better insurance coverage, but she wishes the system were more equitable.
“I have a medical problem,” she said. “It’s not like I did IVF because I wanted to choose the gender.”
One reason CNY is less expensive than other clinics is simply that the privately owned company chooses to charge less, said William Kiltz, its vice president of marketing and business development. Since the company’s beginning in 1997, it has become a large practice with a large volume of IVF cycles, which helps keep prices low.
At this point, more than half its clients come from out of state, and many earn significantly less than a typical patient at another clinic. Twenty percent earn less than $50,000, and “we treat a good number who are on Medicaid,” Kiltz said.
Now that their son, Joaquin, is settled in a good school, Delgado has started working for an agency that provides home health services. After putting in 30 hours a week for 90 days, she’ll be eligible for health insurance.
Michelle Andrews: is a Kaiser Family Health News contributing writer.
andrews.khn@gmail.com, @mandrews110
Hannah Recht: Many losing Medicaid coverage because they don’t complete paperwork

Green states have adopted Medicaid expansion under the Affordable Care Act .
From Kaiser Family Foundation Health News (KFF Health News)
“{W}e need to change up our strategy.’’
— Henry Lipman, New Hampshire’s Medicaid director
More than 600,000 Americans have lost Medicaid coverage since pandemic protections ended on April 1. And a KFF Health News analysis of state data shows the vast majority were removed from state rolls for not completing paperwork.
We have published the underlying reports that contain the data used in this article so that local reporters, researchers, and others can explore state data on Medicaid renewals in more detail.
Under normal circumstances, states review their Medicaid enrollment lists regularly to ensure every recipient qualifies for coverage. But because of a nationwide pause in those reviews during the pandemic, the health insurance program for low-income and disabled Americans kept people covered even if they no longer qualified.
Now, in what’s known as the Medicaid unwinding, states are combing through rolls and deciding who stays and who goes. People who are no longer eligible or don’t complete paperwork in time will be dropped.
The overwhelming majority of people who have lost coverage in most states were dropped because of technicalities, not because state officials determined they no longer meet Medicaid income limits. Four out of every five people dropped so far either never returned the paperwork or omitted required documents, according to a KFF Health News analysis of data from 11 states that provided details on recent cancellations. Now, lawmakers and advocates are expressing alarm over the volume of people losing coverage and, in some states, calling to pause the process.
KFF Health News sought data from the 19 states that started cancellations by May 1. Based on records from 14 states that provided detailed numbers, either in response to a public records request or by posting online, 36 percent of people whose eligibility was reviewed have been disenrolled.
In Indiana, 53,000 residents lost coverage in the first month of the unwinding, 89 percent for procedural reasons like not returning renewal forms. State Rep. Ed Clere, a Republican, expressed dismay at those “staggering numbers” in a May 24 Medicaid advisory group meeting, repeatedly questioning state officials about forms mailed to out-of-date addresses and urging them to give people more than two weeks’ notice before canceling their coverage.
Clere warned that the cancellations set in motion an avoidable revolving door. Some people dropped from Medicaid will have to forgo filling prescriptions and cancel doctor visits because they can’t afford care. Months down the line, after untreated chronic illnesses spiral out of control, they’ll end up in the emergency room where social workers will need to again help them join the program, he said.
Before the unwinding, more than 1 in 4 Americans — 93 million — were covered by Medicaid or CHIP, the Children’s Health Insurance Program, according to KFF Health News’ analysis of the latest enrollment data. Half of all kids are covered by the programs.
About 15 million people will be dropped over the next year as states review participants’ eligibility in monthly tranches.
Most people will find health coverage through new jobs or qualify for subsidized plans through the Affordable Care Act. But millions of others, including many children, will become uninsured and unable to afford basic prescriptions or preventive care. The uninsured rate among those under 65 is projected to rise from a historical low of 8.3% today to 9.3% next year, according to the Congressional Budget Office.
Because each state is handling the unwinding differently, the share of enrollees dropped in the first weeks varies widely.
Several states are first reviewing people officials believe are no longer eligible or who haven’t recently used their insurance. High cancellation rates in those states should level out as the agencies move on to people who likely still qualify.
In Utah, nearly 56 percent of people included in early reviews were dropped. In New Hampshire, 44 percent received cancellation letters within the first two months — almost all for procedural reasons, like not returning paperwork.
But New Hampshire officials found that thousands of people who didn’t fill out the forms indeed earn too much to qualify, according to Henry Lipman, the state’s Medicaid director. They would have been denied anyway. Even so, more people than he expected are not returning renewal forms. “That tells us that we need to change up our strategy,” said Lipman.
In other states, like Virginia and Nebraska, which aren't prioritizing renewals by likely eligibility, about 90 percent have been renewed.
Because of the three-year pause in renewals, many people on Medicaid have never been through the process or aren’t aware they may need to fill out long verification forms, as a recent KFF poll found. Some people moved and didn’t update their contact information.
And while agencies are required to assist enrollees who don’t speak English well, many are sending the forms in only a few common languages.
Tens of thousands of children are losing coverage, as researchers have warned, even though some may still qualify for Medicaid or CHIP. In its first month of reviews, South Dakota ended coverage for 10% of all Medicaid and CHIP enrollees in the state. More than half of them were children. In Arkansas, about 40% were kids.
Many parents don’t know that limits on household income are significantly higher for children than adults. Parents should fill out renewal forms even if they don’t qualify themselves, said Joan Alker, executive director of the Georgetown University Center for Children and Families.
New Hampshire has moved most families with children to the end of the review process. Lipman, the state’s Medicaid director, said his biggest worry is that a child will end up uninsured. Florida also planned to push kids with serious health conditions and other vulnerable groups to the end of the review line.
But according to Miriam Harmatz, advocacy director and founder of the Florida Health Justice Project, state officials sent cancellation letters to several clients with disabled children who probably still qualify. She’s helping those families appeal.
Nearly 250,000 Floridians reviewed in the first month of the unwinding lost coverage, 82 percent of them for reasons like incomplete paperwork, the state reported to federal authorities. House Democrats from the state petitioned Republican Gov. Ron DeSantis to pause the unwinding.
Advocacy coalitions in both Florida and Arkansas also have called for investigations into the review process and a pause on cancellations.
The state is contacting enrollees by phone, email, and text, and continues to process late applications, said Tori Cuddy, a spokesperson for the Florida Department of Children and Families. Cuddy did not respond to questions about issues raised in the petitions.
Federal officials are investigating those complaints and any other problems that emerge, said Dan Tsai, director of the Center for Medicaid & CHIP Services. “If we find that the rules are not being followed, we will take action.”
His agency has directed states to automatically reenroll residents using data from other government programs like unemployment and food assistance when possible. Anyone who can’t be approved through that process must act quickly.
“For the past three years, people have been told to ignore the mail around this, that the renewal was not going to lead to a termination.” Suddenly that mail matters, he said.
Federal law requires states to tell people why they’re losing Medicaid coverage and how to appeal the decision.
Harmatz said some cancellation notices in Florida are vague and could violate due process rules. Letters that she’s seen say “your Medicaid for this period is ending” rather than providing a specific reason for disenrollment, like having too high an income or incomplete paperwork.
If a person requests a hearing before their cancellation takes effect, they can stay covered during the appeals process. Even after being disenrolled, many still have a 90-day window to restore coverage.
In New Hampshire, 13% of people deemed ineligible in the first month have asked for extra time to provide the necessary records. “If you're eligible for Medicaid, we don't want you to lose it,” said Lipman.
Clere, the Indiana state representative, pushed his state’s Medicaid officials during the May meeting to immediately make changes to avoid people unnecessarily becoming uninsured. One official responded that they’ll learn and improve over time.
“I’m just concerned that we’re going to be ‘learning’ as a result of people losing coverage,” Clere replied. “So I don’t want to learn at their expense.”
Hannah Recht is a KFF Health News reporter.
#Medicaid
Judith Graham: In Maine and elsewhere, many elderly struggle to pay for basic necessities

Farmer's market in Monument Square, downtown Portland
— Photo by vBd2media

Townhouses in Portland’s West End, completed in 1835
— Photo by Motionhero
PORTLAND, Maine
Fran Seeley, 81, doesn’t see herself as living on the edge of a financial crisis. But she’s uncomfortably close.
Each month, Seeley, a retired teacher, gets $925 from Social Security and a $287 disbursement from an individual retirement account. To make ends meet, she’s taken out a reverse mortgage on her home here that yields $400 monthly.
So far, Seeley has been able to live on this income — about $19,300 a year — by carefully monitoring her spending and drawing on limited savings. But should her excellent health worsen or she need assistance at home, Seeley doesn’t know how she’d pay for those expenses.
More than half of older women living alone — 54% — are in a similarly precarious financial situation: either poor according to federal poverty standards or with incomes too low to pay for essential expenses. For single men, the share is lower but still surprising — 45%.
That’s according to a valuable but little-known measure of the cost of living for older adults: the Elder Index, developed by researchers at the Gerontology Institute at the University of Massachusetts at Boston.
A new coalition, the Equity in Aging Collaborative, is planning to use the index to influence policies that affect older adults, such as property tax relief and expanded eligibility for programs that assist with medical expenses. Twenty-five prominent aging organizations are members of the collaborative.
The goal is to fuel a robust dialogue about “the true cost of aging in America,” which remains unappreciated, said Ramsey Alwin, president and chief executive of the National Council on Aging, an organizer of the coalition.
Nationally, and for every state and county in the U.S., the Elder Index uses various public databases to calculate the cost of health care, housing, food, transportation and miscellaneous expenses for seniors. It represents a bare-bones budget, adjusted for whether older adults live alone or as part of a couple; whether they’re in poor, good or excellent health; and whether they rent or own homes, with or without a mortgage.
Results from the analyses are eye-opening. In 2020, according to data supplied by Jan Mutchler, director of the Gerontology Institute, the index shows that nearly 5 million older women living alone, 2 million older men living alone, and more than 2 million older couples had incomes that made them economically insecure.
And those estimates were before inflation soared to more than 9% — a 40-year high — and older adults continued to lose jobs during the second and third years of the pandemic. “With those stressors layered on, even more people are struggling,” Mutchler said.
Nationally and in every state, the minimum cost of living for older adults calculated by the Elder Index far exceeds federal poverty thresholds, which are used to calculate official poverty statistics. (Federal poverty thresholds used by the Elder Index differ slightly from federal poverty guidelines. Data for each state can be found here.)
One national example: The Elder Index estimates that a single older adult in good health paying rent needed $27,096, on average, for basic expenses in 2021 — $14,100 more than the federal poverty threshold of $12,996. For couples, the gap between the index’s calculation of necessities and the poverty threshold was even greater.
Yet eligibility for Medicaid, food stamps, housing assistance and other safety-net programs that help older adults is based on federal poverty standards, which don’t account for geographic variations in the cost of living or medical expenses incurred by older adults, among other factors. (This isn’t an issue for older adults alone; the poverty measures have been widely critiqued across age groups.)
“The poverty rate just doesn’t cut it as a realistic look at the struggles older adults are having,” said William Arnone, chief executive officer of the National Academy of Social Insurance, one of the new coalition’s members. “The Elder Index is a reality check.”
In April, University of Massachusetts researchers showed that Social Security benefits cover only a fraction of what older adults need for basic living expenses: 68% for a senior in good health who lives alone and pays rent and 81% for an older couple in the same situation.
“There’s a myth that Social Security and Medicare miraculously take care of all of people’s needs in older age,” said Alwin, of the National Council on Aging. “The reality is they don’t, and far too many people are one crisis away from economic insecurity.”
Organizations across the country have been using the Elder Index to convince policymakers that older adults need more assistance. In New Jersey, where 54% of seniors are economically insecure according to the index, advocates used the data to protect property-tax relief programs for older adults during the pandemic. In New York, where nearly 60% of seniors are economically insecure, advocates persuaded the legislature to raise the Medicaid income eligibility threshold.
In San Diego, where as many as 40% of seniors are economically insecure, Serving Seniors, a nonprofit agency, persuaded county officials to use pandemic-related stimulus payments to expand senior nutrition programs. As a result, the agency has been able to double production of home-delivered meals, to more than 1.5 million annually.
Officials are often wary of the financial impact of expanding programs, said Paul Downey, president and CEO of Serving Seniors. But, he said, “we should be using a reliable measure of economic security and at least know how well the programs we’re offering are doing.” By law, California’s Area Agencies on Aging use the Elder Index in their planning process.
Maine is No. 5 on the list of states ranked by the share of seniors living below the Elder Index, 56%. For someone in Fran Seeley’s situation (an older adult who is in excellent health, lives alone, owns a house, and doesn’t pay a monthly mortgage), the index suggests $22,560 a year is necessary — $3,200 more than Seeley’s annual income and $9,500 above the federal poverty threshold.
Fran Seeley’s income — from Social Security, a retirement account, and a reverse mortgage — comes to about $19,300 a year. With inflation increasing, “it means I have to cut back in any way I can,” Seeley says.
A look at Seeley’s budget reveals how quickly necessary expenses accumulate: $2,041 annually for Medicare Part B (this is deducted from her Social Security check), $4,156 for property and stormwater taxes, $390 for home insurance, $320 for furnace cleaning, $1,440 for heat, $125 for water, $500 for gas and electricity, $300 for property maintenance, $1,260 for phone and Internet, $150 for car registration, $640 for car insurance, $840 for gasoline at current prices, $300 for car maintenance, and $4,800 for food.
The total: $17,262. And that doesn’t include the cost of medications, clothing, toiletries, any kind of entertainment, or other incidentals.
Seeley’s great luxury is caring for four cats, which she describes as “the light of my life.” Their annual wellness checks cost about $400 a year, while their food costs about $1,080.
With inflation now making her budget even tighter, “it means I have to cut back in any way I can. I find myself going into stores and saying, ‘No, I don’t need that,’” Seeley said. “The biggest worry I have is not being able to afford living in my home or becoming ill. I know that medical expenses could wipe me out in no time financially.”
Judith Graham is a Kaiser Health News Reporter.
Phil Galewitz: ACA co-ops soon down to three, including one in Maine

New Mexico Health Connections’ decision to close at year’s end will leave just three of the 23 nonprofit health-insurance co-ops that sprang from the Affordable Care Act.
One co-op serves customers in Maine, another in Wisconsin, and the third operates in Idaho and Montana and will move into Wyoming next year. All made money in 2019 after having survived several rocky years, according to data filed with the National Association of Insurance Commissioners.
They are also all in line to receive tens of millions of dollars from the federal government under an April Supreme Court ruling that said the government inappropriately withheld billions from insurers meant to help cushion losses from 2014 through 2016, the first three years of the ACA marketplaces. While those payments were intended to help any insurers losing money, it was vitally important to the co-ops because they had the least financial backing.
Lauded as a way to boost competition among insurers and hold down prices on the Obamacare exchanges, the co-ops had more than 1 million people enrolled in 26 states at their peak in 2015. Today, they cover about 128,000 people, just 1% of the 11 million Obamacare enrollees who get coverage through the exchanges.
The nonprofit organizations were a last-minute addition to the 2010 health law to satisfy Democratic lawmakers who had failed to secure a public option health plan — one set up and run by the government — on the marketplaces. Congress provided $2 billion in startup loans. But nearly all the co-ops struggled to compete with established carriers, which already had more money and recognized brands.
State insurance officials and health experts are hopeful that the last three co-ops will survive.
“These are the three little miracles,” said Sabrina Corlette, a research professor and co-director of the Center on Health Insurance Reforms at Georgetown University, in Washington, D.C.
Maine Aided in Supreme Court Victory
The Maine co-op, Community Health Options, helped bring competition to the state’s market, which has had trouble at times attracting insurance carriers, said Eric Cioppa, who heads the state’s bureau of insurance.
“The plan has added a level of stability and has been a positive for Maine,” he said.
The co-op has about 28,000 members — down from about 75,000 in 2015 — and is building up its financial reserves, Cioppa said. Community Health Options is one of three insurers in the Obamacare marketplace in Maine, the minimum number experts say is needed to ensure vibrant competition.
Kevin Lewis, CEO of the plan, attributed its survival to several factors, including an initial profit in 2014, the year the ACA marketplaces opened, that put the plan on a secure footing before several years of losses. He also credited bringing most functions of the health plan in-house rather than contracting out, diversifying to sell plans to small and large employers, and securing lower rates from two health systems during a couple of difficult years.
Jay Gould, 60, a member who offers the plan to workers at his small grocery store in Clinton, has been happy with the plan. “They have great customer service, and it’s good to know when I am talking to someone that they are from Maine,” he said.
Central Aroostook Association, a Presque Isle nonprofit that helps children with intellectual disabilities, switched to the co-op last year to save 20% on its health premiums, said administrator Tammi Easler. Having a Maine insurer means any issues can be dealt with quickly, she said. “They are readily available, and I never have to wait on hold for an hour.”
The co-op, which made a $25 million profit each of the past two years, has proposed dropping its average premiums by about 14% in 2021, Lewis said.
Community Health was one of the lead plaintiffs in the case before the Supreme Court and expects to get $59 million in back payments from the settlement.
The federal decision to suspend those so-called risk corridor payments — designed to help health plans recover some of their losses — was one of the factors that caused many of the co-ops to fail, Corlette said. Republican critics of the ACA, however, blame poor management by the plans and lack of oversight by the Obama administration.
Insurers are in talks with the Trump administration about whether the $13 billion due the carriers must be added to their 2020 balance sheet or could be counted toward operations from prior years. This year, insurers are generally banking large profits since many people have delayed non-urgent care because of the COVID-19 pandemic. Since the ACA limits insurers’ profit margins, adding that federal windfall to this year’s ledger might mean many insurers would have to pay out most of the money to their consumers. If the money is applied to earlier years, the insurers could likely keep more of it to add to their reserves.
Too Much Competition in New Mexico
The Supreme Court ruling came too late for New Mexico Health Connections, which lost nearly $60 million from 2015 to 2017. The co-op would have received $43 million in overdue payments, but, in an effort to raise needed cash, it sold that debt to another insurer in 2017 for a much smaller amount.
Marlene Baca, CEO of the co-op, which made a $439,000 profit in 2019, said its goal of bringing competition into the market was achieved, since five other companies will be enrolling customers this fall for 2021. Yet, that competition eventually led to the plan’s decision to end operations, announced last month.
With only 14,000 members, it made no sense to continue operating due to high fixed administrative costs, she said. Her plan was also hurt by the slumping economy this year, which pushed many state residents out of work and made more than 3,000 members eligible for Medicaid, the state-federal health program for the poor.
“We did our very best,” Baca said, noting that her company is closing with enough money to pay its outstanding health claims. Many other co-ops that shuttered were closed out by their states and unable to meet all their debts to health providers, she said.
Montana’s Co-Op Is Expanding
The Mountain Health Co-Op, with about 32,000 members, has just two competitors in its home state of Montana and four in Idaho.
A big factor behind its survival was that the plan received a $15 million loan in 2016 from St. Luke’s Health System, Idaho’s largest hospital provider, said CEO Richard Miltenberger. Although he wasn’t working for the co-op at that time, Miltenberger said, it is his understanding that the hospital wanted to help maintain competition in that marketplace.
The co-op is expecting $57 million from the Supreme Court victory.
“We are in excellent shape,” Miltenberger said. The plan, which paid back the St. Luke’s loan and made a $15 million profit in 2019, added vision benefits this year and is offering a dental exam benefit for next year. It’s also providing most insulin and medications for asthma and chronic obstructive pulmonary disease to members without any copayment to help ensure compliance.
The insurer is moving into Wyoming for 2021, which will end the Blue Cross plan monopoly in that state’s Obamacare marketplace, he said.
Wisconsin’s Mystery Donor
Wisconsin’s Common Ground Healthcare Cooperative was on the verge of ending operations in 2016 when it received a lifesaving $30 million loan, said CEO Cathy Mahaffey. The insurer has refused to identify the benefactor other than to say it was not a person or company doing business with the plan.
In 2018, Common Ground was the only health plan in seven northeastern Wisconsin counties, she said. Today, the co-op has about 54,000 members and faces competition from two to five carriers in the 20 counties where it operates.
Common Ground, which recorded a $73 million profit last year, expects to receive about $95 million from the Supreme Court case victory.
Wisconsin’s decision not to expand Medicaid under the health law has benefited the co-op because people with incomes from 100% to 138% of the federal poverty level ($12,760 to $17,609 for an individual) are ineligible for Medicaid and must stay with marketplace plans for coverage. In states that expanded Medicaid, everyone with incomes under 138% of the poverty level is eligible.
Another factor was its decision in 2016 to eliminate the broad provider network offering and sell a plan offering only a narrow network of doctors and hospitals, allowing it to benefit from lower rates from its providers, according to Mahaffey.
“We are very strong financially,” she said.
Phil Galewitz is a Kaiser Health News reporter.

Julie Appleby: Whither hospital-at-home services after pandemic?

After seven days as an inpatient for complications related to heart problems, Glenn Shanoski was initially hesitant when doctors suggested in early April that he could cut his hospital stay short and recover at home — with high-tech 24-hour monitoring and daily visits from medical teams.
But Shanoski, a 52-year-old electrician in Salem, Mass., decided to give it a try. He’d felt increasingly lonely in a hospital where the COVID-19 pandemic meant no visitors. Also, Boston’s Tufts Medical Center wanted to free up beds for a possible surge of the coronavirus.
With a push from COVID-19, such “hospital-at-home” programs and other remote technologies — from online visits with doctors to virtual physical therapy to home oxygen monitoring — have been rapidly rolled out and, often, embraced.
As remote visits quickly ramped up, Medicare and many private insurers, which previously had limited telehealth coverage, temporarily relaxed payment rules, allowing what has been an organic experiment to proceed.
“This is a once-in-a-lifetime thing,” said Preeti Raghavan, an associate professor of physical medicine and rehabilitation and neurology at Johns Hopkins University School of Medicine, in Baltimore. “It usually takes a long time — 17 years — for an idea to become accepted and deployed and reimbursed in medical practice.”
Physical therapists traded some hands-on care for video-game-like rehabilitation programs patients can do on home computer screens. And hospitals like Tufts, where Shanoski was a patient, sped up preexisting plans for hospital-at-home initiatives. Doctors and patients were often enthusiastic about the results.
“It’s a great program,” said Shanoski, now fully recovered after 11 days of receiving this care. At home, he could talk with his fiancée “and walk around and be with my dogs.”
But what will remain of these innovations in the post-COVID era is now the million-dollar question. There is a need to assess what is gained — or lost — when a service is delivered remotely. Another variable is whether insurers, which currently reimburse virtual visits at the same rate as if they were in person, will continue to do so. If not, what is a proper amount?
It remains to be seen what types of novel remote care will persist from this born-of-necessity experiment.
Said Glenn Melnick, a health-care economist at the University of Southern California who studies hospital systems: “Pieces of it will, but we have to figure out which ones.”
Hospital At Home
Long established in parts of Australia, England, Italy and Spain, such remote programs for hospital care have not caught on here, in large part because U.S. hospitals make money by filling beds.
Hospital-at-home initiatives are offered to stable patients with common diagnoses — like heart failure, pneumonia and kidney infections — who need hospital services that can now be delivered and managed at a distance.
Patients’ homes are temporarily equipped with the necessities, including monitors and communication equipment as well as backup internet and power sources. Care is overseen by health professionals in remote “command centers.”
Medically Home, the private company providing the service for Tufts, sent its own nurses, paramedics and other employees to handle Shanoski’s daily medical care — such as blood tests or consultations via camera with doctors. They inserted an IV and made sure it was working properly during their visits, which often totaled three a day. Even when Medically Home employees were not there, devices monitored Shanoski’s blood pressure and oxygen levels.
For patients transferred from the hospital, like Shanoski, Tufts pays Medically Home a portion of what the hospital receives in payment. For transfers from an emergency room, Medically Home is paid directly by insurers with which it has contracts.
Before the pandemic, at least 20 U.S. health systems had some form of hospital-at-home setup, said Bruce Leff, a professor at Johns Hopkins University School of Medicine who has studied such programs. He said that, for the right patients, they’re just as safe as in-hospital care and can cost 20% to 30% less.
Tele-Rehab?
Glenn Shanoski, a 52-year-old electrician, spent 11 days with hospital-level care at home —– offered by Tufts Medical Center in Boston. Tufts provides daily visits from medical teams to closely monitor patients in their homes. (Courtesy of Glenn Shanoski)
When the coronavirus shut down elective procedures, many physical-therapy offices had to close, too. But a number of patients who had recently had surgery or injuries were at a crucial point in recovery.
Therapists scrambled to set up video capability, while their trade association called insurers and regulators to convince them that remote physical therapy should be covered.
At the end of April, the Centers for Medicare & Medicaid Services added remote physical, speech and occupational therapy to the list of medical services it would cover during the pandemic. Just as it had done for other services, the agency said payment would be the same as for an in-person visit.
Though some patient care cannot be done virtually, such as hands-on manipulation of tight muscles, the doctors discovered many advantages: “When you see them in their home, you can see exactly their situation. Rugs lying around on the floor. What hazards are in the environment, what support systems they have,” said Raghavan, the rehabilitation physician at Johns Hopkins. “We can understand their context.”
Using video links, therapists can assess how a patient moves or walks, for example, or demonstrate home exercises. There are also specially designed video-game programs — similar to Nintendo Wii — that utilize motion sensors to help rehabilitation patients improve balance or specific skills.
“Tele-rehab was very much in the research phase and wasn’t deployed on a wide scale,” Raghavan said. Her department now does 9 out of 10 visits remotely, up from zero before March.
Pneumonia Monitoring
Even before the coronavirus emergency, some patients with mild pneumonia were treated as outpatients.
Now, with hospitals busy with COVID-19 cases and patients eager to minimize unneeded exposure, more physicians are considering this option and for sicker patients. The key is using a small device called a pulse oximeter, which clips onto the end of a finger and measures heart rate, while also estimating the proportion of oxygen in the blood. Costing at most a few hundred dollars, and long common in doctors’ offices, clinics and emergency rooms, the tiny machine can be sent home with patients or purchased online.
“We do it on a case-by-case basis,” said Dr. Gary LeRoy, president of the American Academy of Family Physicians. It’s a good option for relatively healthy patients but is not appropriate for those with underlying conditions that could lead them to deteriorate rapidly, such as heart or lung disease or diabetes, he said.
A pulse oximeter reading of 95% to 100% is considered normal. Generally, LeRoy tells patients to call his office if their readings fall below 90%, or if they have symptoms like fever, chills, confusion, increasing cough or fatigue and their levels are in the 91-to-94 range. That could signal a deterioration that requires further assessment and possibly hospitalization.
“Having a personal physician involved in the process is critically important because you need to know the nuances” of the patient’s history, he said.
What It All Looks Like In The Future
Virtual therapy requires patients or their caregivers to accept more responsibility for maintaining the treatment regimen, and also for activities like bathing and taking medicines. In return, patients get the convenience of being at home.
But the biggest wild card in whether current innovations persist may be how generously insurers decide to cover them. If insurers decide to reimburse telehealth at far less than an in-person visit, that “will have a huge impact on continued use,” said Mike Seel, vice president of the consulting firm Freed Associates in California. A related issue is whether insurers will allow patients’ primary caregivers to deliver treatment remotely or require outsourcing to a distant telehealth service, which might leave patients feeling less satisfied.
The industry’s lobbying group, America’s Health Insurance Plans, said the ongoing crisis has shown that telehealth works. But it offered no specifics on future reimbursement, other than encouraging insurers to “closely collaborate” with local care providers.
Whether virtual therapy is cost-effective “remains to be seen,” said USC’s Melnick. And it depends on perspective: It may be cheaper for a hospital to do a virtual physical therapy session, but the patient might not see any savings if insurance doesn’t reduce the out-of-pocket cost.
Julie Appleby is a Kaiser Health News reporter.jappleby@kff.org, @Julie_Appleby

Shefali Luthra: How insurers sank plan for 'public option' in Connecticut

Headquarters of the huge insurance company Cigna in Bloomfield, Conn
Health-care costs were rising. People couldn’t afford coverage. So, in Connecticut, state lawmakers took action.
Their solution was to attempt to create a public health insurance option, managed by the state, which would ostensibly serve as a low-cost alternative for people who couldn’t afford private plans.
Immediately, an aggressive industry mobilized to kill the idea. Despite months of lobbying, debate and organizing, the proposal was dead on arrival.
“That bill was met with a steam train of opposition,” recalled state Rep. Sean Scanlon, who chairs the legislature’s insurance and real estate committee.
Through a string of presidential debates, the idea of a public option was championed by moderate Democrats ― such as former South Bend, Ind., Mayor Pete Buttigieg, Minnesota Sen. Amy Klobuchar and former Vice President Joe Biden ― as an alternative to a single-payer “Medicare for All” model. Those center-left candidates again touted the idea during the Feb. 25 Democratic debate in South Carolina, with Buttigieg arguing such an approach would deliver universal care without the political baggage. (Buttigieg and Klobuchar have since ended their presidential bids.)
The public option has a common-sense appeal for many Americans who list health-care costs as a top political concern: If the market doesn’t offer patients an affordable health care insurance they like, why not give them the option to buy into a government-run health plan?
But the stunning 2019 defeat of a plan to implement such a policy in Connecticut — a solidly blue, or liberal-leaning, state — shows how difficult it may be to enact even “moderate” solutions that threaten some of America’s most powerful and lucrative industries. The health-insurance industry’s fear: If the average American could weigh a public option — Medicare or Medicaid or some amalgam of the two — against commercial plans on the market, they might find the latter wanting.
That fear has long blocked political action, said Colleen Grogan, a professor at the University of Chicago’s School of Social Service Administration, because “insurance companies are at the table” when health care reform legislation gets proposed.
To be sure, the state calculus is different from what a federal one would be. In the statehouse, a single industry can have an outsize influence and legislators are more skittish about job loss. In Connecticut, that was an especially potent force. Cigna and Aetna are among the state’s top 10 employers.
“They became aware of the bill, and they moved immediately to kill it,” said Frances Padilla, who heads the Universal Health Care Foundation of Connecticut and worked to generate support for the public option.
And those strategies have been replicated at the national level as a national coalition of health industry players ramps up lobbying against Democratic proposals. Beyond insurance, health-care systems and hospitals have joined in mobilizing against both public option and single-payer proposals, for fear a government-backed plan would pay far less than the rates of commercial insurance.
Many states are exploring implementing a public option, and once one is successful, others may well follow, opening the door to a federal program.
“State action is always a precursor for federal action,” said Trish Riley, the executive director of the National Academy for State Health Policy. “There’s a long history of that.”
Virginia state delegate Ibraheem Samirah introduced a new public option bill this session. In Colorado, Gov. Jared Polis is spearheading an effort. And Washington state is the furthest along — it approved a public option last year, and the state-offered plan will be available next year.
But in 2019, Connecticut’s legislators were stuck between two diametrically opposed constituencies, both distinctly local.
Health costs had skyrocketed. Across the state, Scanlon said, small-business owners worried that the high price of insurance was squeezing their margins. A state-provided health plan, the logic went, would be highly regulated and offer lower premiums and stable benefits, providing a viable, affordable alternative to businesses and individuals. (It could also pressure private insurance to offer cheaper plans.)
A coalition of state legislators came together around a proposal: Let small businesses and individuals buy into the state employee health benefit plan. Insurers’ response was swift.
Lobbyists from the insurance industry swarmed the Capitol, recalled Kevin Lembo, the state comptroller. “There was a lot of pressure put on the legislature and governor’s office not to do this.”
State ethics filings make it impossible to tease out how much of Aetna and Cigna’s lobbying dollars were spent on the public option legislation specifically. In the 2019-20 period, Aetna spent almost $158,000 in total lobbying: $93,000 lobbying the Statehouse, and $65,000 on the governor’s office. Cigna spent about $157,000: $84,000 went to the legislature, and $73,000 to the executive.
Anthem, another large insurance company, spent almost $147,000 lobbying during that same period — $23,545 to the governor, and $123,045 to the legislature. Padilla recalled that Anthem also made its opposition clear, though it was less vocal than the other companies. (Anthem did not respond to requests for comment.)
A coalition of insurance companies and business trade groups rolled out an online campaign, commissioning reports and promoting op-eds that argued the state proposal would devastate the local economy.
Lawmakers also received scores of similarly worded emails from Cigna and Aetna employees, voicing concern that a public option would eliminate their jobs, according to documents shared with Kaiser Health News. Cigna declined to comment on those emails, and Aetna never responded to requests for comment.
Connecticut’s first public option bill — which would let people directly buy into the publicly run state employee health plan ― flamed out.
So lawmakers put forth a compromise proposal: The state would contract with private plans to administer the government health option, allowing insurance companies to participate in the system.
The night before voting, that too fell apart. Accounts of what happened vary.
Some say Cigna threatened to pull its business out of the state if a public option were implemented. Publicly, Cigna has said it never issued such a threat but made clear that a public option would harm its bottom line. The company would not elaborate when contacted by KHN.
Now, months later, both Scanlon and Lembo said another attempt is in the works, pegged to legislation resembling last year’s compromise bill. But state lawmakers work only from February through early May, which is not a lot of time for a major bill.
Meanwhile, other states are making similar pushes, fighting their own uphill battles.
“It really depends on whether there are other countervailing pressures in the state that allow politicians to be able to go for a public option,” Grogan said.
And, nationally, if a public option appears to gain national traction, Blendon said, insurance companies “are clearly going to battle.”
They’re going to go after every Republican, every moderate Democrat, to try to say that … it’s a backdoor way to have the government take over insurance,” he said.
Still, when President Barack first proposed the idea of a public option as part of the Affordable Care Act, it was put aside as too radical. Less than a decade later, support for the idea ― every Democratic candidate backs either an optional public health plan or Medicare for All ― is stronger than it ever has been.
So strong, Grogan said, that it is hard for people to understand “the true extent” of the resistance that must be overcome to realize such a plan.
But in Connecticut, politicians say they’re up for a new battle in 2020.
“We can’t accept the status quo. … People are literally dying and going bankrupt,” Scanlon said. “A public option at the state level is the leading fight we can be taking.”
Shefali Luthra is a Kaiser Health News reporter.

Phil Galewitz: Trump's Medicaid chief mostly wrong on its outcomes, access

“This wouldn’t pass muster in a first-year statistics class.’’
— Benjamin Sommers, health-care economist at Harvard, of Medicare-Medicaid chief’s remarks
The Trump administration’s top Medicaid official has been increasingly critical of the entitlement program she has overseen for three years.
Seema Verma, administrator of the Centers for Medicare & Medicaid Services, has warned that the federal government and states need to better control spending and improve care to the 70 million people on Medicaid, the state-federal health insurance program for the low-income population. She supports changes to Medicaid that would give states the option to receive capped annual federal funding for some enrollees instead of open-ended payouts based on enrollment and health costs. This would be a departure from how the program has operated since it began in 1965.
In an early February speech to the American Medical Association, Verma noted how changes are needed because Medicaid is one of the top two biggest expenses for states, and its costs are expected to increase 500% by 2050.
“Yet, for all that spending, health outcomes today on Medicaid are mediocre and many patients have difficulty accessing care,” she said.
Verma’s sharp comments got us wondering if Medicaid recipients were as bad off as she said. So we asked CMS what evidence it has to back up her views.
A CMS spokesperson responded by pointing us to a CMS fact sheet comparing the health status of people on Medicaid to people with private insurance and Medicare. The fact sheet, among other things, showed 43% of Medicaid enrollees report their health as excellent or very good compared with 71% of people with private insurance, 14% on Medicare and 58% who were uninsured.
The spokesperson also pointed to a 2017 report by the Medicaid and CHIP Payment and Access Commission (MACPAC), a congressional advisory board, that noted: “Medicaid enrollees have more difficulty than low-income privately insured individuals in finding a doctor who accepts their insurance and making an appointment; Medicaid enrollees also have more difficulty finding a specialist physician who will treat them.”
We opted to look at those issues separately.
What About Health Status?
Several national Medicaid experts said Verma is wrong to use health status as a proxy for whether Medicaid helps improve health for people. That’s because to be eligible for Medicaid, people must fall into a low income bracket, which can impact their health in many ways. For example, they may live in substandard housing or not get proper nutrition and exercise. In addition, lack of transportation or child care responsibilities can hamper their ability to visit doctors.
Benjamin Sommers, a health economist at Harvard University, said Verma’s comparison of the health status of Medicaid recipients against people with Medicare or private insurance is invalid because the populations are so different and face varied health risks. “This wouldn’t pass muster in a first-year statistics class,” he said.
Death rates, for example, are higher among people in the Medicare program than those in private insurance or Medicaid, he said, but that’s not a knock on Medicare. It’s because Medicare primarily covers people 65 and older.
By definition, Medicaid covers the most vulnerable people in the community, from newborns to the disabled and the poor, said Rachel Nuzum, a vice president with the nonpartisan Commonwealth Fund. “The Medicaid population does not look like the privately insured population.”
Joe Antos, a health economist with the conservative American Enterprise Institute, also agreed, saying he is leery of any studies or statements that evaluate Medicaid without adjusting for risk.
For a better mechanism to gauge health outcomes under Medicaid, experts point to dozens of studies that track what happened in states that chose in the past six years to pursue the Affordable Care Act’s Medicaid expansion. The health law gave states the option to extend Medicaid to everyone with incomes up to 138% of the federal poverty level, or about $17,600 annually for an individual. Thirty-six states and the District of Columbia have adopted the expansion.
“Most research demonstrates that Medicaid expansion has improved access to care, utilization of services, the affordability of care, and financial security among the low-income population,” concluded the Kaiser Family Foundation in summarizing findings from more than 300 studies. “Studies show improved self-reported health following expansion and an association between expansion and certain positive health outcomes.” (Kaiser Health News is an editorially independent program of the foundation.)
Studies found the expansion of Medicaid led to lower mortality rates for people with heart disease and among end-stage renal disease patients initiating dialysis.
Researchers also reported that Medicaid expansion was associated with declines in the length of stay of hospitalized patients. One study found a link between expansion and declines in mechanical ventilation rates among patients hospitalized for various conditions.
Another recent study compared the health characteristics of low-income residents of Texas, which has not expanded Medicaid, and those of Arkansas and Kentucky, which did. It found that new Medicaid enrollees in the latter two states were 41 percentage points more likely to have a usual source of care and 23 percentage points more likely to say they were in excellent health than a comparable group of Texas residents.
Medicaid’s benefits, though, affect far more than the millions of nondisabled adults who gained coverage as a result of the ACA. “Medicaid coverage was associated with a range of positive health behaviors and outcomes, including increased access to care; improved self-reported health status; higher rates of preventive health screenings; lower likelihood of delaying care because of costs; decreased hospital and emergency department utilization; and decreased infant, child, and adult mortality rates,” according to a report issued this month by the nonpartisan Robert Wood Johnson Foundation.
Children — who make up nearly half of Medicaid enrollees — have also benefited from the coverage, studies find. Some studies report that Medicaid contributes to improved health outcomes, including reductions in avoidable hospitalizations and lower child mortality.
Research shows people on Medicaid are generally happy with the coverage.
A Commonwealth Fund survey found 90% of adults with Medicaid were satisfied or very satisfied with their coverage, a slightly higher percentage than those with employer coverage.
Accessible Care?
The evidence here is less emphatic.
A 2017 study published in JAMA Internal Medicine found 84% of Medicaid recipients felt they were able to get all the medical care they needed in the previous six months. Only 3% said they could not get care because of long wait times or because doctors would not accept their insurance.
Verma cites a 2017 MACPAC report that noted some people on Medicaid have issues accessing care. But that report also noted: “The body of work to date by MACPAC and others shows that Medicaid beneficiaries have much better access to care, and much higher health care utilization, than individuals without insurance, particularly when controlling for socioeconomic characteristics and health status.” It also notes that “Medicaid beneficiaries also fare as well as or better than individuals with private insurance on some access measures.”
The report said people with Medicaid are as likely as those with private insurance to have a usual source of care, a doctor visit each year and certain services such as a Pap test to detect cervical cancer.
“Medicaid is not great coverage, but it does open the door for health access to help people deal with medical problems before they become acute,” Antos said.
On the negative side, the report said Medicaid recipients are more likely than privately insured patients to experience longer waiting times to see a doctor. They also are less likely to receive mammograms, colorectal tests and dental visits than the privately insured.
“Compared to having no insurance at all, having Medicaid improves access to care and improves health,” said Rachel Garfield, a vice president at the Kaiser Family Foundation. “There is pretty strong evidence that Medicaid helps patients get the care they need.”
Our Ruling
Verma said that “health outcomes today on Medicaid are mediocre and many patients have difficulty accessing care.”
Numerous studies show people’s health improves as a result of Medicaid coverage. This includes lower mortality rates, shorter hospital stays and more people likely to get cancer screenings.
While it’s hard to specify what “many patients having difficulty accessing care” means, research does show that Medicaid enrollees generally say they have no trouble accessing care most of the time.
We rate the claim as Mostly False.
Phil Galewitz is a Kaiser Health News reporter.
Phil Galewitz: pgalewitz@kff.org, @philgalewitz
Judith Graham: What to do if your home health-care agency ditches you

Craig Holly, of Connecticut, was determined to fight when the home health agency caring for his wife decided to cut off services Jan. 18.
The reason he was given by an agency nurse? His wife was disabled but stable, and Medicare was changing its payment system for home health.
Euphrosyne “Effie” Costas-Holly, 67, has advanced multiple sclerosis. She can’t walk or stand and relies on an overhead lift system to move from room to room in their house.
Effie wasn’t receiving a lot of care: just two visits every week from aides who gave her a bath, and one visit every two weeks from a nurse who evaluated her and changed her suprapubic catheter, a device that drains urine from a tube inserted in the abdomen.
But even that little bit helped. Holly, 71, has a bad back and is responsible for his wife’s needs 24/7. Her urologist didn’t have a lift system in his office and had told the couple it was safer to have Effie’s catheter changed regularly at home.
Holly wasn’t sure what to do. Call his congressman and lodge a complaint? Write a letter to the director of the home health agency owned and operated by Hartford HealthCare Corp., one of the largest health care systems in Connecticut?
Things snapped into focus when Holly attended a late November presentation about Medicare’s home health services by Kathleen Holt, associate director of the Center for Medicare Advocacy.
If you’re told Medicare’s home health benefits have changed, don’t believe it: Coverage rules haven’t been altered and people are still entitled to the same types of services, Holt told the group. (For a complete description of Medicare’s home health benefit, click here.)
All that has changed is how Medicare pays agencies under a new system known as the Patient-Driven Groupings Model (PDGM). This system applies to home health services for older adults with original Medicare. Managed-care-style Medicare Advantage plans, which serve about one-third of Medicare beneficiaries, have their own rules.
Under PDGM, agencies are paid higher rates for patients who need complex nursing care and less for people with long-term chronic conditions who need physical, occupational or speech therapy.
Holly got lucky. When he reached out to Holt, she suggested points to bring up with the agency. Tell them your wife’s urologist wasn’t consulted about a possible discharge from home health, doesn’t agree with this move and is willing to recertify Effie for ongoing home health services, Holt advised.
Within hours, the agency reversed its decision and said Effie’s services would remain in place.
A Hartford HealthCare spokesman said he couldn’t comment on the situation, citing privacy laws. “Our goal is to continue to provide the right care at the right place at the right time with the orders reflecting the specific treatment goals and medical needs of each patient,” he wrote in an email.
“No patients have had services reduced as a result of Medicare’s implementation of the PDGM program.”
But therapists, home health agencies and association leaders say that patients across the country are being told they no longer qualify for certain services (such as vitamin B12 injections or suprapubic catheter changes) or that services have to be cut back or discontinued.
What should you do if this happens to you? Experts have several suggestions:
Get as much information as possible. If your agency says you no longer need services, ask your nurse or therapist what criteria you no longer meet, said Jason Falvey, a physical therapist and postdoctoral research fellow in the geriatrics division at Yale School of Medicine, in New Haven.
Does the agency think skilled services are no longer necessary and that a family member can now provide all needed care? Does it believe the person receiving care is no longer homebound? (To receive Medicare home health services, a person must be homebound and in need of intermittent skilled nursing or therapy services.)
“If the therapist or the agency says that Medicare doesn’t cover a particular service any longer, that should raise red flags because Medicare hasn’t changed its benefits or clinical criteria for home health coverage,” Falvey said.
Enlist your doctor’s help. Armed with this information, get in touch with the physician who ordered home health services for you.
“Your physician should be aware if you feel you’re not getting the services you need,” said Kara Gainer, director of regulatory affairs for the American Physical Therapy Association.
“Doctors should not be sitting on the sidelines; they should be advocating for their patients,” said William Dombi, president of the National Association for Home Care and Hospice.
Take it up the chain of command. Meanwhile, let people at the home health agency know that you’re contesting any decision to reduce or terminate services.
When someone begins home health services, an agency is required to give them a sheet, known as the “Patient Bill of Rights,” with the names and phone numbers of people who can be contacted if difficulties arise. Contact the agency’s clinical supervisor, who should be listed here.
“Call us and trigger a conversation,” said Bud Langham, chief strategy and innovation officer at Encompass Health, which provides home health services to 45,000 patients in 33 states.
Also, contact the organization in your state that oversees home health agencies and let them know you believe your agency isn’t following Medicare’s rules, said Sharmila Sandhu, vice president of regulatory affairs for the American Occupational Therapy Association. This should be among the numbers listed on the bills of rights sheet.
Contact Medicare’s ombudsman. Unlike nursing homes, home health agencies don’t have designated long-term ombudsmen who represent patients’ interests. But you can contact 1-800-Medicare and ask a representative to submit an inquiry or complaint to the general Medicare ombudsman, a spokesman for the Centers for Medicare & Medicaid Services said. The ombudsman is tasked with looking into disputes brought to its attention.
File an expedited appeal. If a home health agency plans to discontinue services altogether, staff are required to give you a “Notice of Medicare non-coverage” stating the date on which services will end, the reason for termination and how to file a “fast appeal.” (This notice must be delivered at least two days before services are due to end.) You have to request an expedited appeal by noon of the day after you receive this notice.
A Medicare Quality Improvement Organization will handle the appeal, review your medical information and generally get back to you within three days. In the meantime, your home health agency is obligated to continue providing services.
Shop around. Multiple home health agencies operate in many areas. Some may be for-profit, others not-for-profit.
“All home health agencies are not alike” and if one agency isn’t meeting your needs “consider shopping around,” Dombi said. While this may not be possible in smaller towns or rural areas, in urban areas many choices are typically available.
Contact an advocate. The Center for Medicare Advocacy has been hearing from patients who are being given all kinds of misinformation related to Medicare’s new home health payment system.
Among the things that patients have been told, mistakenly: “Medicare ‘closed a loophole’ as of Jan. 1 so your care will no longer be provided after mid-January,” “Medicare will no longer pay for more than one home health aide per week,” and “We aren’t paid sufficiently to continue your care,” said Judith Stein, the center’s executive director.
Some agencies may not understand the changes that Medicare is implementing; confusion is widespread. Advocates such as the Center for Medicare Advocacy (contact them at here) or the Medicare Rights Center (national help line: 800-333-4114) can help you understand what’s going on and potentially intervene on your behalf.
Judith Graham is a Kaiser Health News journalist.
Patty Wright: Newly blue Maine expands access to abortion
The Maine State House, designed by Charles Bulfinch, and built 1829–1832. Bullfinch also designed the famous Massachusetts State House, with its iconic gold dome.
While abortion bans in Republican-led states dominated headlines in recent weeks, a handful of other states have expanded abortion access. Maine joined those ranks in June with two new laws ― one requires all insurance and Medicaid to cover the procedure and the other allows physician assistants and nurses with advanced training to perform it.
With these laws, Maine joins New York, Illinois, Rhode Island and Vermont as states that are trying to shore up the right to abortion in advance of an expected U.S. Supreme Court challenge. What sets Maine apart is how recently Democrats have taken power in the state.
“Elections matter,” said Nicole Clegg of Planned Parenthood of Northern New England. Since the 2018 elections, Maine has its largest contingent of female lawmakers, with 71 women serving in both chambers. “We saw an overwhelming majority of elected officials who support reproductive rights and access to reproductive health care.”
The dramatic political change also saw Maine elect its first female governor, Janet Mills, a Democrat who took over from Paul LePage, a Tea Party stalwart who served two terms. LePage had blocked Medicaid expansion in the state even after voters approved it in a referendum.
Clegg and other supporters of abortion rights hailed the new abortion legislation: “It will be the single most important event since Roe versus Wadein the state of Maine.”
Taken together, the intent of the two laws is to make it easier for women to afford and to find abortion care in the largely rural state.
Nurse practitioners like Julie Jenkins, who works in a small coastal town, said that increasing the number of abortion providers will make it easier for patients who now have to travel long distances in Maine to have a doctor perform the procedure.
“Five hours to get to a provider and back ― that’s not unheard of,” Jenkins said.
Physician assistants and nurses with advanced training will be able to perform a surgical form of the procedure known as an aspiration abortion. These clinicians already are allowed to use the same technique in other circumstances, such as when a woman has a miscarriage.
Maine’s other new law, set to be implemented early next year, requires all insurance plans ― including Medicaid ― to cover abortions. Kate Brogan of Maine Family Planning said it’s a workaround for a U.S. law known as the Hyde Amendment that prohibits federal funding for abortions except to save the life of the woman, or if the pregnancy arises from incest or rape.
“[Hyde] is a policy decision that we think coerces women into continuing pregnancies that they don’t want to continue,” Brogan said. “Because if you continue your pregnancy, Medicaid will cover it. But if you want to end your pregnancy, you have to come up with the money [to pay for an abortion].”
State dollars will now fund abortions under Maine’s Medicaid, which is funded by both state and federal tax dollars.
Though the bill passed in the Democratic-controlled legislature, it faced staunch opposition from Republicans during floor debates including Sen. Lisa Keim.
“Maine people should not be forced to have their hard-earned tax dollars [used] to take the life of a living pre-born child,” said Keim.
Instead, Keim argued, abortions for low-income women should be funded by supporters who wish to donate money; otherwise, the religious convictions of abortion opponents are at risk. “Our decision today cannot be to strip the religious liberty of Maine people through taxation,” Keim said during the debate.
Rep. Beth O’Connor, a Republican who says she personally opposes abortion but believes women should have a choice, said she had safety concerns about letting clinicians who are not doctors provide abortions.
“I think this is very risky, and I think it puts the woman’s health at risk,” O’Connor said.
In contrast, advanced practice clinicians say the legislation, which will take effect in September, said this law merely allows them to operate to the full scope of their expertise and expands access to important health care. The measure has the backing of physician groups like the Maine Medical Association.
Just as red-state laws restricting abortion are being challenged, so are Maine’s new laws. Days after Maine’s law on Medicaid abortion passed, organizations that oppose abortion rights announced they’re mounting an effort to put the issue on the ballot for a people’s veto.
This story is part of a partnership that includes Maine Public Radio, NPR and Kaiser Health News. Patty Wright is a reporter at Maine Public Radio.
Nicole Braun: The GOP's war on democracy in the Heartland
From OtherWords.org
For millions of Americans, there’s no “making it” if you fall beneath a certain social class line. And the Michigan GOP, which was roundly rejected in the last election, is determined to keep it that way.
In neighboring Wisconsin, Republicans decided to show voters there that their voices, votes, hardships, and pain don’t matter. They passed a series of lame-duck bills making it all but impossible for newly elected Democrats to implement their agenda.
Here in Michigan, the GOP quickly followed suit. Republicans pushed many bills through the legislature in their last days in office that hurt regular folks but benefit the elite, despite election results that show unambiguously what voters want.
Among many other things, these egregious bills ignore voter-approved sick leave protections and minimize wage increases, make it more difficult to vote, restrict campaign finance reform measures, and — for good measure — make it harder for voters to get future proposals on the ballot.
The GOP doesn’t care how tough many folks in Michigan have it, and there’s no apparent logic to their thinking except to make it tougher.
For instance, earlier Medicaid rules passed by Michigan Republicans say that folks need to work 20 hours a week. But often when you work 20 hours a week, you no longer qualify for Medicaid — even if you still can’t afford private insurance.
And when you work 20 hours a week without insurance and get sick, you’re out of luck — because Republicans just gutted a citizen-passed initiative to make sure workers have paid sick leave.
They also pushed forward a bill to drastically slow down minimum wage increases approved by voters. Studies show that no one in America can afford a two-bedroom apartment anywhere working even full-time for minimum wage, but Republicans watered down the voter-approved increase anyway.
Outgoing Republican Gov. Rick Snyder signed those bills. Sadly, many folks I talked to weren’t surprised.
Folks in Michigan have been suffering for years under GOP rule. We’ve seen blatant power abuses, including the undemocratic recall of elected officials. We’ve seen rising inequality, a rampant opioid crisis, poverty, corruption, and egregious failures like the Flint water crisis.
“Our governor has a body count — the kids he killed in Flint,” said Wil Gallivan, who lives outside Flint.
“Expecting him to all of a sudden gain some decency is just wishful thinking. We should all be wearing yellow vests at the Capitol, 100,000 people strong,” he added, referring to the “yellow vest” protests rocking France. “But who can afford to take time off their jobs to do that?”
Recalling Snyder’s purchase of an exorbitantly expensive cake just as news of the Flint water crisis was breaking, former bartender and Flint native Carol Frey reflected: “People who pull that usually lack the compassion and empathy chip.”
I teach sociology. It’s a given that the more inequality there is, the more violence, anger, despair, addiction, and hatred there is too. Inequality produces unhealthy humans and unhappy communities. No one can bloom in such unhealthiness.
By pushing forward these harmful bills even after a progressive wave, Michigan Republicans are saying that the people who voted them out don’t matter. So are their neighbors in Wisconsin and in other states across the country (like Florida, where lawmakers are trying to water down a voter-passed initiative to give people who serve time their vote back).
Still, more protests and acts of resistance are planned. Michigan people are strong, and we fight back — even if we’re broke and tired.
Nicole Braun is a sociologist in northern Michigan.
Peter Certo: GOP's mid-terms campaign depended on lies, fear-mongering and rule-rigging

This 1874 cartoon by Thomas Nast is considered the first important portrayal of the Republican elephant.
Via OtherWords.org
I can’t be the only one who spent the night of the mid-terms tossing and turning. Though I managed to shut off the coverage and try to sleep, spasms of anxiety woke me repeatedly throughout the dreary hours.
Ultimately, Republicans picked off several Red State Senate seats while Democrats won back the House and at least seven governorships.
A Democratic House will serve as a badly needed check after two years of aggressive Republican monopoly, but I can’t help feeling uneasy. For one thing, I can’t shake the last days of the campaign.
For a while, Republicans “merely” lied about their policy agenda.
Rather than campaigning on the $2 trillion tax cut for rich people they actually passed, they promised a middle class tax cut they never even had a bill for. And after spending all last year trying to throw 20 million to 30 million Americans off their health care, they (unbelievably!) promised to defend Americans’ pre-existing condition coverage — even as they actively sought to undermine it.
But the lies took a much darker turn as the White House took hold of the narrative.
Led by the president, GOP propagandists turned a few thousand refugees — over a thousand miles away in southern Mexico — into an “invading army.” The White House put out an ad about it so shockingly racist and false that even Fox News stopped airing it.
Unashamed, President Trump kept repeating the obvious lie that the homeless refugees were funded by Jewish philanthropist George Soros — even after a refugee-hating extremist murdered 11 Jews at a Pittsburgh synagogue.
Such vile hatred may have been key to Red State Republican gains in the Senate. But where that wasn’t enough, it was backstopped by voter suppression and gerrymandering.
Suppression may have helped the GOP governor candidates fend off strong challenges in Florida and especially Georgia, where tens of thousands of voters were scrubbed from the rolls and lines in Democratic precincts ran up to five hours long.
And thanks to gerrymandering, it took an extraordinary effort for Democrats to win even a slim House majority. They’re up only a few seats despite decisively winning the popular vote by at least 9 points. Had it been “only” a 4 or 5 point win, Vox’s Matthew Yglesias estimates, the GOP might have retained its majority.
Also worth noting: Democratic Senate candidates actually racked up over 10 million more votes than Republicans, even as Republicans picked up Senate seats on a GOP-tilting map,
To me these results show that Republicans can’t win with their actual policy agenda — not even in many Red States, judging by some ballot initiative results.
For instance, Red State voters in Missouri and Arkansas raised their minimum wages against the wishes of state Republicans. Missouri also legalized medicinal marijuana, along with deeply conservative Utah, and Purple State Michigan voters brought legal recreational marijuana to the Midwest.
Along with Utah, ruby red Idaho and Nebraska expanded Medicaid under Obamacare, a big win for health care.
These progressive policies are far more popular than their right-wing alternatives. So Republicans rely on a potent combination of lies, fear-mongering, and rule-rigging to win.
If Democrats ever hope to really come in from the wilderness, they need to support a host of radical pro-democracy reforms.
In that they can take inspiration from a stunning movement in Florida, where voters re-enfranchised over 1 million of their neighbors with felony convictions. And from Michigan, Colorado, Utah and Missouri, which all passed initiatives to support citizen-led redistricting. And from Maryland, Michigan, and Nevada, which all made voter registration easier.
Uneasiness is part and parcel of drawing breath in 2018. But if I sleep a little better tonight, it’ll be thanks to movements like those.
Peter Certo is the editorial manager of the Institute for Policy Studies and the editor of OtherWords.org.

Judith Graham: Mainers to vote on expanding home health care, to be paid for by new tax

By JUDITH GRAHAM
As Election Day draws near, a ballot initiative in Maine to provide universal home care is shining a spotlight on the inadequacies of the nation’s long-term-care system. The essential problem: Although most older adults want to live at home when their health starts to decline or they become frail, programs that help them do so are narrow in scope, fragmented and poorly funded. Medicare’s home care benefits are limited to seniors and adults with disabilities who are homebound and need skilled services intermittently.
State Medicaid programs vary widely but are generally restricted to people at the lower end of income ladder. Long-term-care insurance is expensive and covers only a small slice of the older population. That leaves millions of middle-class families struggling to figure out what to do when an older relative develops a serious chronic illness, such as heart failure, or suffers an acute medical crisis, such as a stroke. “We’re about to have the largest older population we’ve ever had, which is going to need exponentially more care than has ever been needed before. And we’re not prepared,” said Ai-jen Poo, co-director of Caring Across Generations, an organization working to expand long-term care services across the U.S. Maine, with nearly 20 percent of its residents age 65 and older, is exploring a radical response to this dilemma that’s being closely watched by other states.
Its ballot initiative, known as Question 1, proposes that home care services be available to all residents, at no cost, regardless of income. If enacted, it would become the first such program in the nation. Adults would be eligible for the program when they need help with at least one “activity of daily living”: walking, bathing, dressing, eating, toileting, personal hygiene and getting in or out of bed. Services covered would include care from aides and companions; speech, physical and occupational therapy; counseling; home repairs; transportation; respite care; devices for people with disabilities; and even, occasionally, small rent subsidies. Stipends would be granted to family caregivers. Seventy-seven percent of program funds would be directed to home care aides, in a move to strengthen this workforce.
More than 21,000 people could qualify for home care services under the new program, in addition to about 5,600 people who already receive services through Maine Medicaid and other state programs, according to the most definitive analysis to date, published last month by researchers at the University of Southern Maine’s Muskie School of Public Service.
Funding for the new program would come from a new 3.8 percent tax on wages and non-wage income that isn’t taxed by Social Security: a threshold of $128,400 per person in 2018. Between $180 million and $310 million would be raised annually, according to various estimates. The program would be fully implemented by January 2022. The political battle over Question 1 is fierce, although no one questions the need for affordable home care for seniors and people with disabilities.
In AARP’s most recent “Long-Term Services and Supports State Scorecard,” Maine ranked last in the nation on affordability of home care. Among thousands of people affected are Rick Alexander of Blue Hill, Maine. 70, a retired school librarian, and his wife, Debbie, 64, who has multiple sclerosis.
“Since Debbie has a progressive form of MS, her needs are going to increase,” said Alexander, his wife’s sole, unpaid caregiver and a supporter of Question 1. “We brought in some paid help years back, but we couldn’t do that for very long: It’s too expensive.” Alexander wants to keep Debbie at home as long as possible, but he worries about the physical demands and emotional consequences.
“I have chronic clinical depression and periodically I go down into the dumps, a long way,” he admitted. “When that happens, it’s hard for me to motivate myself to do anything.” Also, it’s generally accepted in Maine that something needs to be done about a severe shortage of home care aides — a problem surfacing nationwide. Each week, 6,000 hours of home care services that have been authorized aren’t delivered by Maine agencies because of staff shortages, which are particularly acute in rural areas, according to the Maine Council on Aging.
Despite these areas of consensus, however, disagreements surrounding Question 1 are intense and most Maine health care and business associations oppose it, along with all four candidates for governor.
Taxes are a key point of contention. Question 1 supporters argue that a relatively small number of high-income individuals would pay extra taxes. The Maine Center for Economic Policy estimates that only 3.4 percent of people earning income in Maine would be affected, according to a September report. Citing ambiguous language in the initiative, opponents argue that families earning more than $128,400 would also be subject to the tax hike, significantly expanding its impact. A pressing concern is that higher taxes would discourage doctors, nurses and other professionals from moving to or remaining in Maine.
“We have a workforce crisis already, and this increase — which would make our income tax rate among the highest in the country — would be a disaster,” said Jeffrey Austin, vice president of government affairs at the Maine Hospital Association. The program is too expansive and expensive to be sustained long term, other opponents say.
“We have limited public resources in Maine and those should be dedicated to the people most in need, fiscally and physically,” said Newell Augur, a lobbyist for the Home Care & Hospice Alliance of Maine and chair of the “NO on Question One/Stop the Scam” campaign.
In a statement, AARP Maine, which has not taken a stand on Question 1, expressed reservations. “Using a payroll tax to pay for HCBS [home and community-based services] is an untested policy at the local level,” it noted. Also controversial is the board that would be established to operate the home care program. The initiative calls for nine members (three from home care agencies, three direct care workers and three service recipients) elected by constituent organizations to oversee the program.
“The board wouldn’t be accountable to the governor or the legislature, and Maine taxpayers would have no say over how their money is being spent,” said Jacob Posik, a policy analyst at the conservative-leaning Maine Heritage Policy Center. Supporters note that an advisory committee would include state officials from multiple agencies. The board’s structure is meant to be “responsive to the people providing and receiving the care,” said Mike Tipping, communications director for the Maine People’s Alliance, a grass-roots organization that’s spearheading Question 1 and that helped pass a 2017 ballot initiative expanding Medicaid in Maine, currently tied up in the courts.
For all these policy disputes, it’s clear that Question 1 has considerable emotional resonance. “I’ve never had people cry signing a petition and tell me how much something like this would have changed their lives,” said Kevin Simowitz, political director for Caring Across Generations. One of the people who’s spoken out publicly is the Rev. Myrick Cross, 75, of St. Patrick’s Episcopal Church in Brewer. Cross works part time at the church so he can pay for aides that care for his 38- year-old daughter with Down syndrome and his 95-year-old mother, who has suffered from kidney disease, falls, wounds that didn’t heal and pneumonia in the past several years.
Cross works part time at the church so he can pay for aides that care for his 38-year-old daughter with Down syndrome and his 95-year-old mother, who has suffered from kidney disease, falls, wounds that didn’t heal and pneumonia in the past several years. “I will do whatever I need to keep them home,” he said.
Originally, Cross looked to home care agencies for assistance, but with rates of $23 to $25 per hour “that was more than I could afford,” he said. Today, three local residents provide more than 50 hours of care a week for $12 to $15 an hour.
“I’m blessed that I’m able to work and to hire all these people to keep us going,” Cross said. “But several members of my congregation are older and don’t have the family resources that we have. This would make the quality of their lives better.”
Martha Burk: A sad birthday for Medicare and Medicaid
Via OtherWords.org
July 30 marks a very important anniversary in our modern political history.
Fifty-three years ago in 1965, President Lyndon Johnson signed Medicare and Medicaid into law, creating two programs that would disproportionately improve the lives of older and low-income Americans — especially women.
Fast-forward to 2018, and both programs are very much under siege. Nowhere is the struggle starker than in the House Republican budget — titled “A Brighter American Future” — now on Capitol Hill.
The importance of Medicare as a source of women’s health coverage can’t be over-emphasized.
Older and disabled women make up more than half the total beneficiaries, and two-thirds of those 85 and over. This budget from hell takes a giant step toward privatizing the program by allowing insurance companies into the Medicare marketplace, which means benefits could be caught in a race to the bottom and become too paltry to cover all but the barest of medical needs.
Medicaid is the joint federal-state program that provides low-income people with health care. The proposed Republican budget repeals the Medicaid expansion that came with Obamacare, which will cause 14 million to 17 million people to lose coverage.
The Medicaid remnants that survive would be turned into block grants, allowing states to pick and choose who gets covered and what kind of benefits they get — no doubt with little or no federal oversight. That approach makes it easier to cut the program without saying how many people would be dropped, or how much benefits would be lowered.
Since poor women under retirement age and their children are the biggest group of beneficiaries, it stands to reason they’d also be the biggest losers.
But there’s more. Because women have more chronic health conditions like arthritis, hypertension, and osteoporosis, they’re more likely to need institutional care. Since Medicare generally doesn’t cover nursing home care, Medicaid provides such care for those with disabilities and/or very low incomes — and 60 percent of those folks are women.
What’s not in the budget? Long gone is the Obama-era effort close the Gingrich-Edwards tax loophole that allows some high-income individuals (possibly including Donald Trump) to avoid Medicare and Social Security payroll taxes altogether, resulting in billions of lost revenue for both programs.
The House Republican budget probably won’t pass in its present form. But with Republican majorities in both houses of Congress, even compromises are sure to favor more cuts.
“A Brighter American Future?” Hardly. This summer’s 53rd anniversary of Medicare and Medicaid looks like a less than happy one for those that depend on them most — namely women, but really anyone counting on growing older.
Martha Burk is the director of the Corporate Accountability Project for the National Council of Women’s Organizations (NCWO) and the author of the book Your Voice, Your Vote.
And handy for congressional insider trading
From Robert Whitcomb's "Digital Diary,'' in GoLocal24.com:
Congress, at least in recent sessions, has not particularly cared about poor people with limited access to medical care. As Robert Pear noted in The New York Times, “They cannot agree on subsidies for low-income people under the Affordable Care Act or even how to extend funding for the broadly popular Children’s Health Insurance Program.’’ Many Republicans have often expressed a barely disguised distaste for Medicaid and the low-income people on it, while they’re leery of offending the generally higher-income and high-voting folks on Medicare, a much more expansive program.
Most members of the House and Senate are affluent and have few interactions with poor people who are uninsured and who can’t afford doctor visits or prescription drugs.
But the solons do love expanding funding for medical research, with a plan, for example to boost the funding of the National Institutes of Health by $2 billion in the next fiscal year. Mr. Pear notes, accurately in my view, that a major reason could be that legislators think that the research could create cures for ailments that they, their families and friends might have. And of course, few legislators are young; ailments increase with age.
“{T}he cynic in me says it’s because of the prevalence of selfishness. We all want to know there’s something out there that will cure us if we need it, but many of us are quite reluctant to pay for somebody else to get cured when they need it,’’ R. Alta Charo, a law and bioethics professor at the University of Wisconsin, told The Times.
I think that there’s another element in Congress’s love of funding medical research and development: Legislators may see this as a way of getting in early on investments in the drug and medical-device sectors. Enjoy a bit of insider trading. For guidance on such lucrative activities, consult, for example, former Georgia Congressman and former Health and Human Services Secretary Tom Price, M.D.
To read The Times’s story, please hit this link.
LeeAnne Hall: Many have jobs BECAUSE they're on Medicaid
On Jan. 11, the Trump administration issued a cruel announcement: If you can’t find a job, don’t count on being able to get health care.
Under an unprecedented new policy, the administration will let states kick people off Medicaid for the crime of being unemployed. Instead of providing good jobs to struggling people, the administration is offering threats and tougher times.
Those hurt could include the Carrier plant workers from Indiana, whose jobs Trump promised to save when he was campaigning for the presidency. Last year, the company announced 600 layoffs.
Now the last of these employees are being pushed out the door. One worker says she’s “a lost paycheck away from homeless.”
Imagine telling her Medicaid won’t be there for her on top of everything else she’ll lose. The heartlessness is incomprehensible.
Still, her state’s governor is one of ten that’s jumping on the administration’s new proposal to require work or work-related activities. Kentucky’s plan has already been approved.
This is no way to treat people you claim to care about — especially when lawmakers can improve our lives with policies providing child care, paid family and medical leave, and living-wage jobs in a clean-energy economy, to say nothing of affordable health care for all.
Simple facts show that this work requirement isn’t about jobs. Most working-age adults who use Medicaid already work, and many of them have jobs thanks to Medicaid — not despite it.
That’s because Medicaid helps them get and stay healthy enough to work. After Ohio expanded Medicaid, three quarters of those who signed up said getting coverage helped them get work. In Michigan, more than two-thirds also said it helped better at a job they already had.
This policy is another blow for those facing racial or other discrimination on the job. It punishes people in job-scarce communities. It hurts people struggling to find work when they have a past criminal conviction.
And, while the administration says people with disabilities won’t be affected, that could be by only by the strictest definition of disability. Those who’ve been hurt on the job won’t necessarily be protected. Neither may many people struggling with addiction, mental health concerns, or physical conditions that make working difficult or impossible.
We can see from Kentucky’s plan what this could look like. New premiums for struggling families. Paperwork lockouts. A financial or health “literacy test” reminiscent of tests that barred African American people from voting. State officials say 90,000-95,000 people will lose their coverage.
Last year, Americans demanded we not go backwards on health care. Thousands of us showed up at town halls to block the GOP effort to repeal the Affordable Care Act and the gutting of Medicaid.
Everyone should get the care they need.
The expansion of Medicaid under the Affordable Care Act was a step in that direction. It gave many of us hope for the country we can be: one where a family’s fortunes don’t depend on the good graces of a giant corporation, and our lives don’t depend on the size of our wallet.
We still have a long way to go. Many are shut out of health care because of citizenship status, because coverage is still too expensive, or because our states refuse to expand Medicaid.
But the Trump administration and GOP Congress are moving us backward. This new Medicaid scheme is just part of it. There’s also the recent tax bill that will raise insurance premiums while giving huge cuts to corporations like Carrier — which, according to one employee facing layoffs, is “getting money hand over fist.”
Americans want health care expanded, not taken away. They can’t trick us with yet another scheme. Let’s raise our voices again and protect Medicaid.
LeeAnn Hall is the co-director of People’s Action and a member of the executive committee of Health Care for America Now. Distributed by OtherWords.org.
David Warsh: The sleazy Sacklers' lethal painkiller promotions and the need for a 'Health Fed'
President Trump has declared the opioid crisis a public health emergency, rather than a national emergency, since the Federal Emergency Management Agency is over-extended in dealing with storm relief. Unfortunately, the Hospital Preparedness and Public Health Emergency Funds are equally strapped for cash, running respectively at 50 percent and 30 percent below their peak levels of a decade ago. Congress will have to act.
It was, therefore, an especially good time for “The Family that Built an Empire of Pain,” to appear last week in The New Yorker. You can read Patrick Radden Keefe’s remarkable story about the wellsprings of the crisis for free online, more easily, if less pleasurably, than in the magazine itself. The sub-head states, “The Sackler dynasty’s ruthless marketing of painkillers has generated billions of dollars – and millions of addicts.”
Others have worked on the Sackler family story over the years, documenting its leading role in producing the opioid epidemic, including Barry Meier, of The New York Times, who first uncovered the extensive marketing efforts for OxyContin, and the Los Angeles Times team that documented the "12-Hour Problem '' that Keefe describes. But none has achieved anything like the rhetorical force of Keefe’s article. Once it is reworked as a book, I expect that “Empire of Pain” will eventually attain the status of Rachel Carson’s Silent Spring, Jane Jacobs’s The Death and Life of Great American Cities, and other classics of social criticism. It is an astonishing story. You might as well read it now.
The three brothers of the Sackler family — Arthur (1913-87), Mortimer (1916-2010), and Raymond (1920-2017) – are far better known as philanthropists than as pharmaceutical entrepreneurs. All three attended medical school and subsequently worked together at Creedmoor Psychiatric Center, in Queens, N.Y. Arthur put himself through medical school working for William Douglas McAdams, a small advertising agency specializing in medical markets, then bought the business. In 1952, the three physicians bought Purdue Frederick, a little manufacturer of patent medicines in Greenwich Village (and no relation to the famous university). Each owned a third.
While Mortimer and Raymond built the company, Arthur took a more distant role, concentrating on medicine as editor in chief of the Journal of Clinical and Experimental Psychopathology from 1950-1962. In 1960, he founded a biweekly newspaper, Medical Tribune, which eventually reached 600,000 subscribers.
The Sackler family grew tolerably rich on the sale of Valium, which between 1969 and 1982 was the top-selling pharmaceutical drug in the United States. When Sen. Estes Kefauver (D.-Tenn.) investigated the rapidly growing pharmaceutical industry in the early 1960s, a staff member prepared a memo that read, in part,
"The Sackler empire is a completely integrated operation in that it can devise a new drug in its drug development enterprise, have the drug clinically tested and secure favorable reports on the drug from various hospitals with which they have connections, conceive the advertising approach and prepare the actual advertising copy with which to promote the drug, have the clinical articles as well as the advertising copy published in their own medical journals, [and] prepare and plant articles in newspapers and magazines.''
Enter Raymond’s son Richard Sackler (b. 1945), in 1971, fresh out of medical school. Starting as assistant to his father, during the next 30 years he presided over efforts to develop OxyContin and turn it into the best-selling pain medicine in the world. How the company, re-named Purdue Pharma, managed that forms the bulk of Keefe’s 13,000-word account.
Simply put, thanks to massive marketing efforts, the long-lasting narcotic came to be widely prescribed, not just for severe pain associated with surgery or cancer, but for almost any discomfort, including arthritis, back pain and sports injuries – despite its obviously addictive properties. Early versions turned out to be ruinously easy to abuse; later editions turned out to be a gateway to the use of cheaper heroin. More than 300,000 lives have been lost to overdoses of opioid drugs since 2000; perhaps 10 times as many have been shattered.
Arthur’s heirs sold their father’s share of the company to his brothers sometime after 1987. Mortimer moved to Europe to spend and save his dividends Raymond ran the company day-to day for many years, and died only last July. Nine family members are among the directors of the private company. Past president Richard Sackler was deposed last year, as part of Kentucky’s complaint that many of Purdue’s marketing methods were illegal. A battle to unseal his testimony has ensued. Many more lawsuits are in train; their tactics resemble the campaign to rein in the use of tobacco. Congress can be expected to again hold hearings.
The editorial board of The Wall Street Journal also addressed the topic, uncharacteristically ignoring the supply side in favor of demand factors, in a piece headlined "The Opioid Puzzle'' (subscription required). The editorial board’s interest was piqued by “the government’s role is allowing too-easy access to painkillers, particularly among society’s poor and vulnerable.”
Medicaid recipients receive prescriptions for twice as much pain medication as those not covered by the government’s low-income plan, the editors wrote, citing government figures. And one out of every three Medicare beneficiaries received opioid prescriptions last year, half a million of them in extravagant doses. “The only way to explain this cascade of pills is an epidemic of fraud,” the editors concluded.
Better to put the two analyses together. OxyContin sales are estimated to have been around $35 billion over the last 20 years. An enormous portion of that was surely paid by the government as insurance subsidies. Only when you see the two programs unfolding together do you begin to comprehend the nature of the problem – the entrepreneurial genius of the Sackler family on the one hand, developing and marketing popular mood-altering and painkilling drugs since the 1950s; on the other, the rise of government medical insurance since 1966, when the Medicare program went into effect.
Throw in the mostly unrecognized extent to which big pharmaceutical manufacturers have discouraged all manner of research on the painkilling applications of medical marijuana, and you have a real witches’ brew.
The U.S . health-care industry may be, in certain respects, the best in the world; certainly it is the most expensive. As the opioid epidemic demonstrates, it offers a colossal field for mischief. The editorial board of the WSJ is right about this much: innovation is the answer, to the opioid crisis, and much else among the medical sector’s many other ills. In this case the desideratum is regulation – not Pentagon-style hierarchy, but rather the decentralized and consensual decision-making represented by the Federal Reserve System.
The blueprint developed 10 years ago by former Senate Majority Leader Tom Daschle (D.-South Dakota) in his run-up to a presidential campaign that was ultimately overtaken by that of the junior senator from Illinois, Barack Obama, is still the only model that make sense. Daschle imagined a dozen or so regional health-care authorities, sharing power among regulators, physicians, hospitals, insurers, device and pharmaceutical providers, governed by a federal board of governors insulated as much as possible from politics.
A Health Care Fed eventually will deliver efficiency – and diminish freebooting – in the enormous sector, in much the same way the Federal Reserve Board stabilized the similarly turbulent banking industry a hundred years ago. It’s just going to take more time – another generation or two, I would guess.
David Warsh, a long time financial columnist and an economic historian, is proprietor of economic principals. com, where this first appeared.
Patty Wright: Maine governor puts brakes on Medicaid expansion

Maine State House, in Augusta.
Just hours after Maine voters became the first in the nation to use the ballot box to expand Medicaid under the Affordable Care Act, Republican Gov. Paul LePage said he wouldn’t implement it unless the Legislature funds the state’s share of an expansion.
“Give me the money and I will enforce the referendum,” LePage said. Unless the Legislature fully funds the expansion — without raising taxes or using the state’s rainy day fund — he said he wouldn’t implement it.
LePage has long been a staunch opponent of Medicaid expansion. The Maine Legislature has passed bills to expand the insurance program five times since 2013, but the governor vetoed each one.
That track record prompted Robyn Merrill, co-chair of the coalition Mainers for Health Care, to take the matter directly to voters Tuesday.
The strategy worked. Medicaid expansion, or Question 2, passed handily, with 59 percent of voters in favor and 41 percent against.
“Maine is sending a strong and weighty message to politicians in Augusta, and across the country,” Merrill said. “We need more affordable health care, not less.”
Medicaid expansion would bring health coverage to about 70,000 people in Maine.
As a battle now brews over implementation in Maine, other states will likely be watching: groups in Idaho and Utah are trying to put Medicaid expansion on their state ballots next year.
With passage of the ballot measure, Maine is poised to join the 31 states and the District of Columbia that have already expanded Medicaid to cover adults with incomes up to 138 percent of the federal poverty level. That’s about $16,000 dollars for an individual, and about $34,000 for a family of four.
Currently, people in Maine who make too much for traditional Medicaid and who aren’t eligible for subsidized health insurance on the federal marketplace fall into a coverage gap. It was created when the Supreme Court made Medicaid expansion under the Affordable Care Act optional.
That’s the situation Kathleen Phelps finds herself in. She’s a hairdresser from Waterville who has emphysema and chronic obstructive pulmonary disease. She said she has had to forgo her medications and oxygen because she can’t afford them. “Finally, finally, maybe people now people like myself can get the health care we need,” she said.
Medicaid expansion would also be a win for hospitals. More than half of those in Maine are operating in the red. Across the state, hospitals provide more than $100 million a year in charity care, according to the Maine Hospital Association. Expanding Medicaid coverage will bolster their fiscal health and give doctors and nurses more options to treat their formerly uninsured patients, said Jeff Austin, a spokesman with the association.
“There are just avenues of care that open up when you see a patient from recommending a prescription drug or seeing a counselor,” he said. “Doors that were closed previously will now be open.”
But voter approval may not be enough. Though a legislative budget analysis office estimates Medicaid expansion would bring about $500 million in federal funding to Maine each year, it would also cost the state about $50 million a year.
The fate of the Medicaid expansion will now be in the hands of the Legislature, where lawmakers can change it like any other bill. Four ballot initiatives passed by Maine voters last year have been delayed, altered or overturned.
But state Democratic leaders pledge to implement the measure. “Any attempts to illegally delay or subvert the law … will be fought with every recourse at our disposal,” Speaker of the House Sara Gideon said. “Mainers demanded affordable access to health care yesterday, and that is exactly what we intend to deliver.”
Patty Wright is a journalist for Maine Public.
This story is part of a partnership that includes Maine Public, NPR and Kaiser Health News.

Jill Richardson: America's service workers need healthcare
Via OtherWords.org
Our country has a powerful myth that anyone can succeed as long as he or she works hard.
That’s the story of Alexander Hamilton that has swept Broadway: how a “bastard orphan” can become “a hero and a scholar.” According to the lyrics he did it by working harder, being smarter, and being a self-starter.
If that’s all you need to do to succeed, then it’s your own fault if you’re poor.
And White House spokeswoman Kellyanne Conway has no sympathy for you. If you’re sad the Republicans want to take away your Medicaid, she says you can go get a job. Because your poverty is your own fault.
To quote Ernest Hemingway at the end of The Sun Also Rises, “Isn’t it pretty to think so?”
The reality isn’t as nice. We don’t live in a society where anyone can get ahead just by working hard. It might feel that way if you grew up middle class, but that’s not the reality that millions of Americans live in.
Sociological research confirms this unpleasant truth again and again.
As for the people on Medicaid who should just “get a job,” odds are that they already have a job. Maybe two jobs.
We as a society want people working in restaurants, cleaning our hotel rooms, checking us out and stocking shelves at stores, and doing any number of low-skilled, generally low-wage jobs. Some people even oppose giving those workers a raise because it would either cut into corporate profits or raise prices.
Well, we can’t have it both ways. We can’t benefit from low-wage labor while simultaneously blaming low-wage workers for their own poverty.
And if you’re truly callous enough not to care if the working poor have access to affordable health care, consider how their plight affects you.
Suppose for a moment that 22 million Americans lose their health care, which is what the Congressional Budget Office predicted would happen if the Senate passed the dead-for-now Republican healthcare bill. What happens?
Those 22 million people no longer go for preventive check ups. They don’t treat medical problems when they occur, before the problems get worse. They wait until they have no choice, and then they go to the emergency room.
If they cannot pay the bills accrued at the emergency room, the hospital eats the cost. But hospitals must balance their budgets somehow, so they raise prices for everyone else.
If you’re insured, then you’re not paying the hospital directly, so the higher prices go to your insurance company. And they pass it on to you in the form of higher premiums.
Thus, if you aren’t moved by the human suffering caused by depriving the working poor of health care, perhaps you’ll be moved by your own pocketbook.
Unless emergency rooms start declining treatment to anyone who can’t pay, turning cancer patients and gunshot victims onto the streets to die, somebody is going to pay for the care of the uninsured.
The question is whether they’ll be able to go for preventive check-ups and treat problems early, or whether they ‘ll go to the emergency room after they can no longer avoid it.
For those who rely on Obamacare for their insurance — myself included — the prospects of losing their healthcare is terrifying. I have several friends with cancer who are literally afraid they will die if a repeal bill passes. And that’s not hyperbole.
It’s time we stopped telling ourselves that anyone who’s struggling only has themselves to blame. And as the wealthiest nation on earth, it’s a travesty that we aren’t willing to help them.
Jill Richardson is the author of Recipe for America: Why Our Food System Is Broken and What We Can Do to Fix It.
Peter Certo: Forget Russia, what about Trump's collusion with U.S. corporations?
Via OtherWords.org
I've always been a little skeptical that there’d be a smoking gun about the Trump campaign’s alleged collusion with Russia. The latest news about Donald Trump, Jr., however, is tantalizingly close.
The short version of the story, revealed by e-mails that The New York Times obtained, is that the president’s eldest son was offered “some official documents and information that would incriminate Hillary” and “would be very useful to your father.”
More to the point, the younger Trump was explicitly told this was “part of Russia and its government’s support for Mr. Trump.” Donald, Jr.’s reply? “I love it.”
Trump Jr. didn’t just host that meeting at Trump Tower. He also brought along campaign manager Paul Manafort and top Trump confidante (and son-in-law) Jared Kushner.
We still don’t have evidence they coordinated with Russian efforts to release Clinton campaign emails, spread “fake news,” or hack state voting systems. But at the very least, the top members of Trump’s inner circle turned up to get intelligence they knew was part of a foreign effort to meddle in the election.
Some in Washington are convinced they’ve heard enough already, with Virginia Sen, (and failed VP candidate) Tim Kaine suggesting that meeting might be called “treason.”
Perhaps. But it’s worth asking: Who’s done the real harm here? Some argue thatit’s not the Russians after all.
“The effects of the crime are undetectable,” the legendary social critic Noam Chomsky says of the alleged Russian meddling, “unlike the massive effects of interference by corporate power and private wealth.”
That’s worth dwelling on.
Many leading liberals suspect, now with a little more evidence, that Trump worked with Russia to win his election. But we’ve long known that huge corporations and wealthy individuals threw their weight behind the billionaire.
That gambit’s paying off far more handsomely for them — and more destructively for the rest of us — than any scheme by Putin.
The evidence is hiding in plain sight.
The top priority in Congress right now is to move a health bill that would gut Medicaid and throw at least 22 million Americans off their insurance — while loosening regulations on insurance companies and cutting taxes on the wealthiest by over $346 billion.
As few as 12 percent of Americans support that bill, but the allegiance of its supporters isn’t to voters — it’s plainly to the wealthy donors who’d get those tax cuts.
Meanwhile, majorities of Americans in every single congressional district support efforts to curb local pollution, limit carbon emissions, and transition to wind and solar. And majorities in every single state back the Paris climate agreement.
Yet even as scientists warn large parts of the planet could soon become uninhabitable, the fossil fuel-backed Trump administration has put a climate denier in charge of the EPA, pulled the U.S. out of the Paris Accord, and signed legislation to let coal companies dump toxic ash in local waterways.
Meanwhile, as the administration escalates the unpopular Afghan war once again, Kushner invited billionaire military contractors — including Blackwater founder Erik Prince — to advise on policy there.
Elsewhere, JPMorgan CEO Jamie Dimon and other architects of the housing crash are advising Trump on financial deregulation, while student-debt profiteers set policy at the Department of Education.
Chomsky complains that this sort of collusion is often “not considered a crime but the normal workings of democracy.” While Trump has taken it to new heights, it’s certainly a bipartisan problem.
If Trump’s people did work with Russia to undermine our vote, they should absolutely be held accountable. But the politicians leading the charge don’t have a snowball’s chance of redeeming our democracy unless they’re willing to take on the corporate conspirators much closer to home.
Peter Certo is the editorial manager of the Institute for Policy Studies and the editor of OtherWords.org.
Trump's 'pluto-populism'
Adapted from an item in Robert Whitcomb's "Digital Diary'' in GoLocal24.com
The Trump budget proposal is filled with so many bogus assumptions and so much creative accounting it’s hard to take any of it seriously. Indeed, people in both parties on Capitol Hill are treating it as a joke.
But there is a central, cohering direction – make America’s put-upon rich people even richer while sticking it to poorer people, many of whom, deluded by Trump’s demagoguery and such right-wing propaganda organs as Fox “News,’’ voted for the mogul. (Meanwhile, many Democrat-inclined people were too lazy tomake it to the polls.) You have to give the hateand fake-conspiracy peddlers at Fox credit – the network has very good production values.
Of course, the richer the rich get, the more they control the government and the more that they’re able to further enrich themselves in a vicious or at least lucrative circle.
An essential part of the Trump budget is the assumption, or, rather, assertion, that it will somehow be paid for by increased economic growth – more of what George H.W. Bush used to call “voodoo economics.’’ The promise is that annual gross domestic product growth will rise to 3 percent, even as the nonpartisan Congressional Budget Office projects only a 1.9 percent rate. That’s because the CBO technicians wisely take into consideration, among other things, our aging population and falling productivity.
Most administrations – including Obama’s – havecooked (or massaged?) the books and often projected considerably higher GDP growth than happens. But the assumptions in the Trump plan are particularly egregious given the Niagara of retiring Baby Boomers and the big proposed tax cuts.
For many Boomers, by the way – especially the richer ones -- Trump is relatively kindly. Older white Baby Boomers vote heavily Republican, and he has vowed not to touch gigantically expensive Medicare or regular Social Security – by far the two biggest entitlement programs – which of course benefit them.
He promised in the campaign not to cut Medicaid. Now he wants to slash Medicaid, Food Stamps and Social Security Disability Insurance. That isn’t to say that Medicaid can’t use some major improvements, such as reducing the amount of unnecessary care and in some cases including work requirements for recipients. And Social Security Disability Insurance has long been rife with abuse. But the fact is that most of the people who benefit from these programs are honest and truly needy. Indeed, most are far more honest than Donald Trump.
Martin Wolf, a Financial Times columnist, described Trump’s “ideology’’ well when he called it “pluto-populism” -- “policies that benefit plutocrats, justified by populist rhetoric.”